Valérie had covered all the bases. Gluten-free diet, dairy-free, soy-free. Selenium, zinc, and vitamin D supplements. Complete intestinal protocol. Stress management. Her anti-TPO antibodies had dropped from 800 to 400 in a year. But for six months, they had stalled. Despite everything she was doing, despite the rigor of her protocol, the antibodies refused to drop below 400. When I asked her if she had any dental problems, she looked at me with surprise. “My teeth? What do they have to do with my thyroid?”
The connection is direct, documented, and almost never explored in consultations. Valérie had untreated chronic periodontitis, four old dental amalgams, and she had been using fluoridated toothpaste for thirty years. Her mouth was a permanent infectious, toxic, and inflammatory focus that was feeding her thyroid autoimmunity just as surely as gluten or stress. And no one had ever asked her about it.
“Dental infectious foci are the most frequent and most overlooked entry points for chronic diseases.” Alexandre Salmanoff
Salmanoff wrote this in the 1950s. Dentists of that era already knew the concept of “infectious focus at a distance”: a chronic dental infection that causes symptoms in distant organs through bacterial dissemination via the blood. Seventy years later, research confirms what Salmanoff observed clinically: the mouth is the primary entry portal for autoimmune triggers, and the thyroid, located just below, is the first target.
Your mouth speaks to your thyroid
The mouth is the most colonized organ in the human body after the intestines. More than 700 bacterial species coexist in the oral cavity, on the teeth, gums, tongue, and tonsils. In balance, this oral flora is protective. It produces antimicrobial substances, modulates pH, and constitutes a first line of immune defense. But when this balance is disrupted by insufficient hygiene, by chronic use of antiseptic mouthwashes, by a sugar-rich diet, or by a weakened immune system, pathogenic bacteria gain the upper hand.
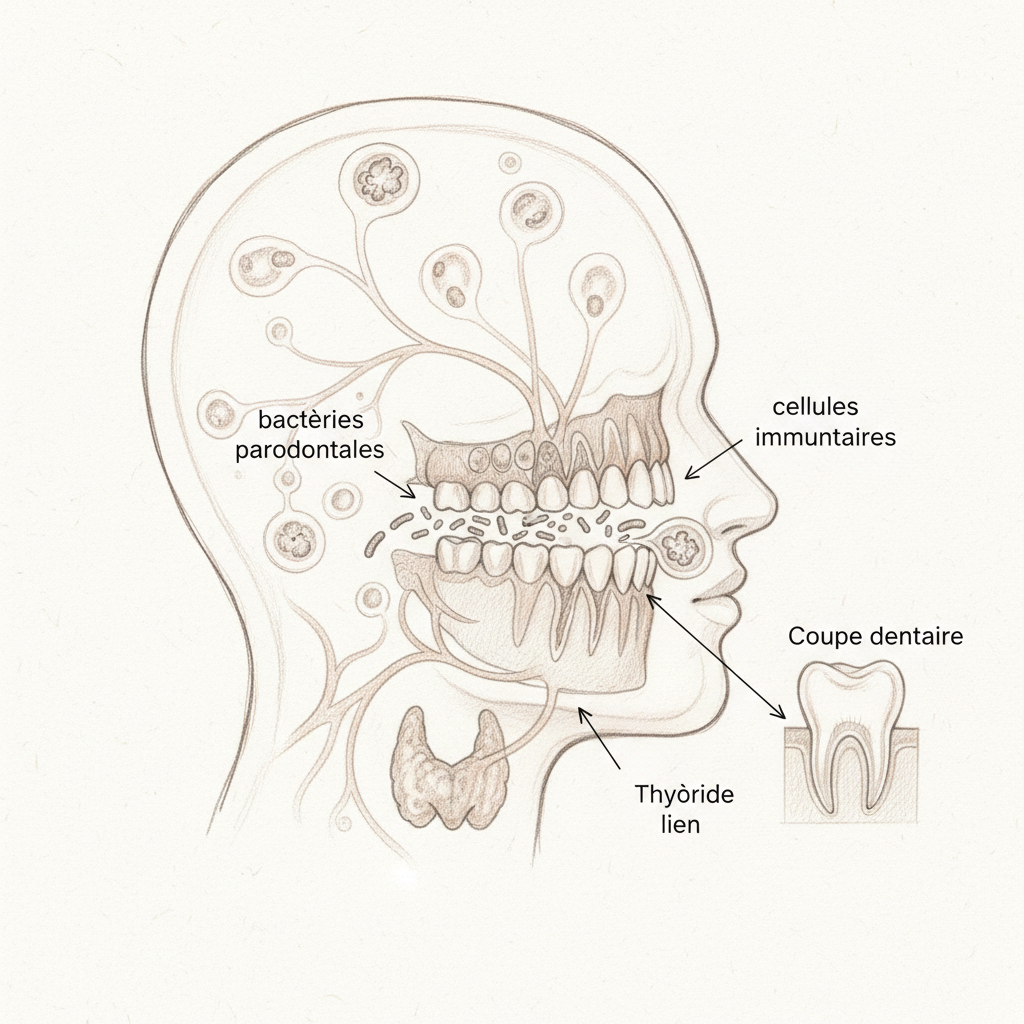
What makes the mouth-thyroid connection so powerful is anatomical proximity and vascular richness. The thyroid is located in the neck, just below the mandible. It shares part of its lymphatic drainage with the ENT sphere. And the oral mucosa, extremely well-vascularized, allows rapid passage of bacteria and their toxins into the general circulation. Each tooth brushing, each vigorous chewing, and especially each dental procedure causes transient bacteremia: oral bacteria pass into the blood. In a healthy person, the immune system neutralizes them within minutes. In a person whose immune system is already in hypervigilant mode due to Hashimoto, these bacteria can trigger an inflammatory cascade that stimulates anti-thyroid antibodies.
Periodontitis: the silent trigger
Periodontitis is a chronic infectious disease of the tissues supporting the tooth: the gum, the periodontal ligament, and the alveolar bone. It affects nearly 50 percent of adults over thirty to varying degrees, and its prevalence increases with age. It is the leading cause of tooth loss in adults. But it is also, and this is much less known, a cardiovascular risk factor, an aggravating factor for diabetes, and a potential trigger for autoimmunity.

The link between periodontitis and Hashimoto is documented by recent studies showing a statistically significant correlation between periodontitis severity and anti-TPO antibody levels. The mechanism operates through several pathways. Chronic bacteremia sends periodontal bacteria into the blood repeatedly, which stimulates the production of pro-inflammatory cytokines IL-6 and TNF-alpha. These cytokines are the same ones elevated in Hashimoto. They increase intestinal permeability (again), stimulate antibody production, and promote the conversion of T4 to reverse T3.
There is also molecular mimicry. Certain bacterial proteins from periodontal pathogens present amino acid sequences similar to those of thyroid proteins. The immune system, mounting a defense against these bacteria, produces antibodies that also recognize thyroid proteins and attack them. It is the same mechanism as gliadin-thyroglobulin mimicry in the case of gluten, but this time the culprit comes from the mouth.
Signs of periodontitis are often subtle: gums bleeding when brushing, redness of the gingival margin, persistent bad breath, gingival recession (teeth appear longer), tooth mobility. Many patients consider bleeding gums when brushing to be “normal.” It is not normal. It is a sign of active infection sending bacteria into your blood with each brushing.
Fluoride and cell death
Fluoride is added to most commercial toothpastes at concentrations of 1000 to 1500 ppm (parts per million). Its role is to strengthen tooth enamel by forming fluorapatite, more resistant to acids than natural hydroxyapatite. That is its benefit. Its cost is what it does to your thyroid.
Fluoride is a halogen, like iodine, bromine, and chlorine. These four elements compete for the same receptors in the body. Fluoride, when absorbed (and some of the fluoride in toothpaste is absorbed through the oral mucosa), competes with iodine for the NIS transporters (sodium-iodide symporter) in the thyroid. It blocks iodine uptake, reducing thyroid hormone synthesis. But it does worse: at certain concentrations, fluoride causes direct cell death of thyrocytes, the cells that make up the thyroid gland. This is not theory. It is documented cellular toxicology.
Sources of fluoride are multiple: toothpaste (the most obvious), tap water in regions where water is fluoridated, fluoridated mouthwashes, fluoride dental treatments, black tea (the tea plant naturally accumulates fluoride), and certain medications. For Hashimoto patients, replacing fluoridated toothpaste with hydroxyapatite toothpaste (which protects enamel without fluoride’s drawbacks) is a simple, inexpensive step that can be potentially significant over the long term.
Amalgams and heavy metals
Dental amalgams, those gray-silver fillings many of us have had in our mouths since childhood, contain approximately 50 percent metallic mercury. Mercury is a neurotoxin, nephrotoxin, and proven endocrine disruptor. And contrary to what was long claimed, amalgams are not inert. They continuously release mercury in vapor form, especially during chewing of hot foods, during brushing, and during bruxism (teeth grinding at night).
Inhaled mercury passes into the lungs, enters the bloodstream, crosses the blood-brain barrier, and accumulates in target organs: brain, kidneys, and thyroid. In the thyroid, mercury interferes with hormone synthesis, stimulates autoimmune antibody production, and creates oxidative stress that damages glandular cells. Detoxification of heavy metals is a complex topic beyond the scope of this article, but one point is crucial: amalgam removal must be performed by a dentist trained in the SMART (Safe Mercury Amalgam Removal Technique) protocol. This protocol includes the use of a dental dam, high-powered suction, nasal oxygen, and an isolated operative field to prevent the patient from inhaling or swallowing mercury particles during removal. An unsecured removal can cause massive mercury release that worsens autoimmunity instead of relieving it.
X-rays: the overlooked risk

The thyroid is one of the most radiosensitive organs in the body. It is located directly in the radiation field of panoramic dental X-rays (orthopantomograms) and cone beam scanners. Each panoramic dental X-ray exposes the thyroid to a dose of radiation. For a healthy person, this dose is low and probably inconsequential. But for a person whose thyroid is already under autoimmune attack, each additional exposure is a potential aggravating factor.
The solution is disarmingly simple: request a leaded thyroid collar (thyroid protector) during any dental X-ray. This device exists, is available in all dental offices, is free, and takes only two seconds to install. Yet in my experience, it is rarely offered spontaneously. It is up to the patient to ask for it. So ask for it. With every panoramic, with every retroalveolar X-ray, with every dental scanner. Protect your thyroid.
What to do concretely
Marchesseau classified oral hygiene among the fundamentals of “detoxification treatment,” alongside diet and physical activity. For him, the mouth was the first emunctory, the first place of contact between the organism and the outside world. The quality of this first contact largely determined the quality of the terrain downstream.
First action: replace your fluoridated toothpaste with a fluoride-free toothpaste. Hydroxyapatite (HAp) toothpastes are an effective and safe alternative. Hydroxyapatite is the natural component of tooth enamel. It remineralizes teeth without the endocrine effects of fluoride. Powdered green clay is another option, used for generations in naturopathy.
Second action: stop daily antiseptic mouthwashes. The chlorhexidine and alcohol in conventional mouthwashes destroy not only pathogenic bacteria but also the protective bacteria that maintain the balance of oral flora. By destroying this flora, you create conditions for oral dysbiosis that promotes periodontitis and infections. Oil pulling, a mouthwash with virgin coconut oil practiced for ten minutes in the morning on an empty stomach, is an alternative that reduces pathogenic bacterial load without destroying commensal flora. It is an ancestral Ayurvedic practice that modern research is beginning to validate.
Third action: consult a periodontist for a complete evaluation. A simple periodontal probing (measuring the depth of gingival pockets) allows you to know if you have periodontitis. If so, periodontal treatment (deep scaling, root planing) can significantly reduce bacterial load and the systemic inflammation that feeds your antibodies.
Valérie had her four amalgams removed by a dentist trained in the SMART protocol. She treated her periodontitis. She replaced her toothpaste with a hydroxyapatite formula. Six months later, her anti-TPO antibodies had dropped from 400 to 280. The plateau she couldn’t break through for months had given way, simply by treating a focus that no one had addressed. The mouth. The forgotten portal of autoimmunity.
Do you want to explore the overlooked causes of Hashimoto? This article reviews all the triggers, including those that conventional medicine doesn’t look at.
To go further
To deepen your understanding of detoxification, read Liver detoxification and methylation, NAC and glutathione, and The forgotten causes of Hashimoto. To understand the role of terrain in autoimmunity, Salmanoff and the body’s plumbing is an enlightening read.




Laisser un commentaire
Sois le premier à commenter cet article.