Thomas is fifty-five years old and has had Hashimoto on Levothyrox 75 mcg for twelve years. His TSH is well controlled, his T3 and T4 are within normal ranges, but he retains residual fatigue, intermittent brain fog and chilliness that Levothyrox has never completely corrected. His endocrinologist tells him that his tests are “perfect” and there is nothing more to do. Thomas has resigned himself to the idea that this is “just how it is” with Hashimoto.
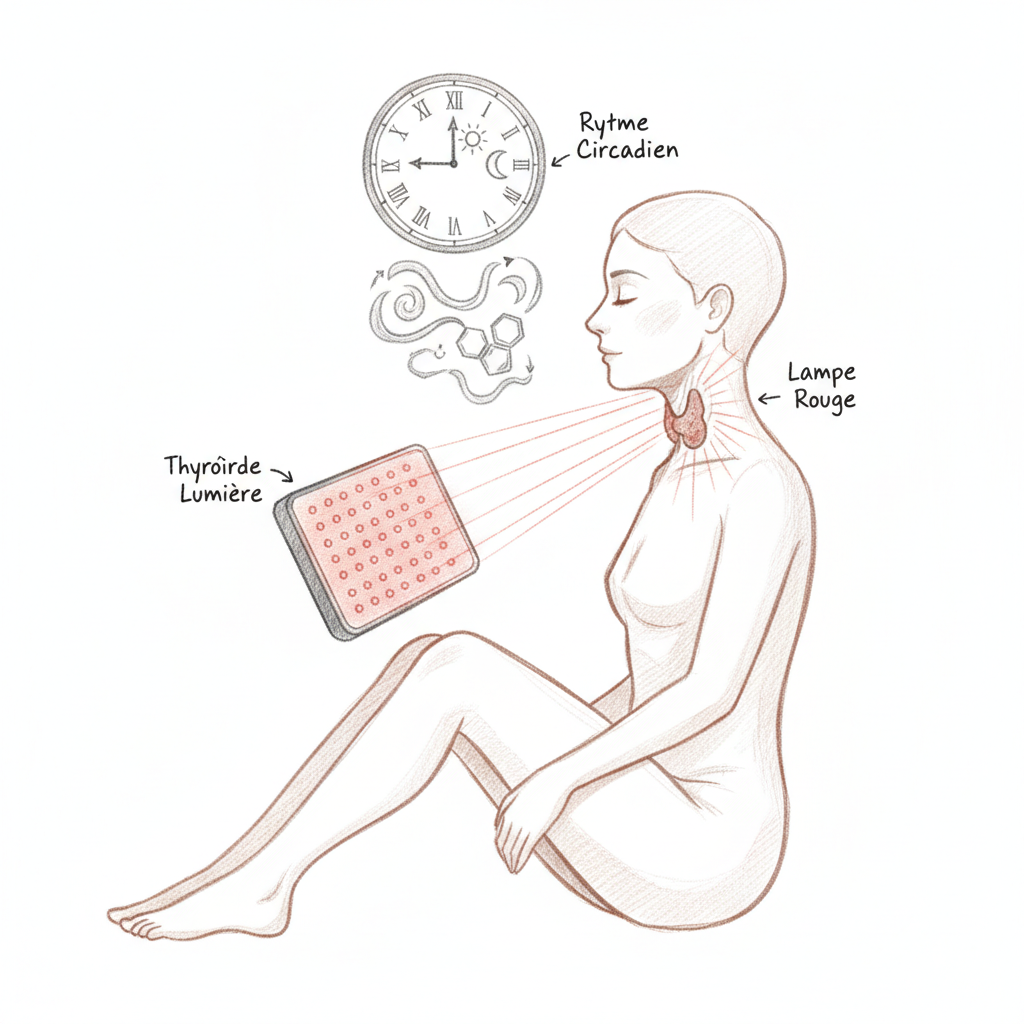
I proposed two light-based interventions to him. The first: a 10,000 lux light therapy lamp in the morning at breakfast, thirty minutes, to resynchronize his circadian rhythm (his morning cortisol was flattened at 5.2 nmol/L when the functional norm is above 15). The second: a photobiomodulation device (red light 660 nm) applied directly to the thyroid, twice weekly for ten weeks.

After three months, the results were there. His morning energy had increased noticeably (he no longer needed three coffees to “get going”). His morning cortisol had risen to 11.8 nmol/L. And his endocrinologist had to reduce his Levothyrox from 75 to 62.5 mcg because his free T3 was starting to rise above normal. Thomas’s thyroid, after twelve years of autoimmune disease, was showing signs of functional recovery.
Photobiomodulation: medicine through light
Photobiomodulation (PBM), formerly called LLLT (Low-Level Laser Therapy), is the use of red light (620-700 nm) and near-infrared (700-1100 nm) at low power to stimulate cellular regeneration, reduce inflammation and relieve pain. It is not a marginal “alternative” therapy: over 5,000 studies published in peer-reviewed journals document its effects, and it has been used in dermatology, rheumatology, dentistry and sports medicine since the 1990s.
The primary mechanism is mitochondrial. Red and near-infrared light is absorbed by cytochrome c oxidase, complex IV of the mitochondrial respiratory chain. This absorption releases nitric oxide (NO) that was blocking the enzyme, which restarts ATP production (cellular energy), stimulates the production of growth factors and modulates the inflammatory response via controlled production of reactive oxygen species (ROS) that serve as signaling molecules.
In simple terms: red light “wakes up” tired mitochondria and allows them to produce more energy. For a thyroid gland damaged by chronic autoimmunity, whose cells are inflamed, infiltrated with lymphocytes and whose mitochondria are dysfunctional, this stimulation can make the difference between a gland that continues to deteriorate and a gland that begins to regenerate.
Studies on the thyroid
The most cited study is that of Höfling et al. (2013, Brazil), a placebo-controlled randomized trial on 43 Hashimoto patients on Levothyrox. The protocol consisted of two sessions per week for ten weeks, with an 830 nm laser (near-infrared) applied to the thyroid for 40 seconds per point, on four points distributed over the two thyroid lobes.
The results were remarkable. In the treated group, 47% of patients were able to reduce their Levothyrox dose. Twenty percent were able to stop Levothyrox completely while maintaining normal TSH. Anti-TPO antibodies decreased significantly. And ultrasound showed improvement in thyroid vascularization. These results were maintained at nine-month follow-up.
Other studies, primarily Brazilian and Russian, confirmed these results with wavelengths of 630-670 nm (visible red). The proposed mechanisms are reduction in lymphocyte infiltration (less autoimmune attack), stimulation of neovascularization (better gland irrigation), reduction in local pro-inflammatory cytokines and stimulation of thyrocyte regeneration (thyroid cells).
Circadian rhythm: the other light that matters
Before discussing therapeutic red light, we must discuss natural light and circadian rhythm. TSH follows a pronounced circadian rhythm: it is maximal between 2am and 4am (during deep sleep) and minimal in late afternoon. This rhythm is synchronized by the circadian clock of the suprachiasmatic nucleus, itself synchronized by morning light entering through the eyes.
When circadian rhythm is disrupted (night work, chronic jet lag, evening screen exposure, lack of natural morning light), TSH secretion becomes disorganized, morning cortisol is flattened (which worsens thyroid fatigue) and residual morning melatonin delays metabolic “startup.”
This is why morning light therapy (10,000 lux for twenty to thirty minutes upon waking) is a therapeutic tool in its own right for thyroid patients. It resynchronizes nocturnal TSH, restores the morning cortisol peak (which improves energy and T4 to T3 conversion, since cortisol is a cofactor of deiodinase), and improves the quality of sleep the following night (by advancing evening melatonin secretion).
Hertoghe, in his approach to functional endocrinology, considers light management to be as important as dietary management for hormonal health. “We live in a society of permanent artificial light in the evening and darkness in the morning. It is exactly the opposite of what our biology expects. And our hormones pay the price.”
The complete light protocol
The circadian component (daily) includes bright light exposure in the morning within thirty minutes of waking. Either natural light (going outside, even on cloudy days, as 10,000 lux corresponds to an overcast day) or a certified 10,000 lux light therapy lamp, placed 30-40 cm from the face for twenty to thirty minutes (during breakfast for example). In the evening, reduce blue light exposure after 8pm (night mode on screens, blue light blocking glasses, dimmed and warm lighting).
The photobiomodulation component (two to three times per week) uses a red LED device (660 nm) or near-infrared (850 nm), with a power of 30 to 50 mW/cm2. Apply directly to the anterior neck, over the thyroid, for one to three minutes per side (right and left lobes). The optimal distance is 1 to 5 cm from the skin. Sessions are preferably done in the morning or early afternoon (not in the evening, as cellular stimulation can disrupt sleep). The initial protocol is ten weeks, two to three sessions per week, with a thyroid panel check at the end.
The natural light exposure component (daily) is the simplest and most neglected: spend time outdoors. Sunlight contains the entire spectrum (blue light in the morning for circadian synchronization, red and infrared light constantly for cellular stimulation). Thirty to sixty minutes outdoors per day, without sunglasses in the morning (morning UV is weak and retinal cells need direct light to synchronize the clock), is a free and powerful therapeutic tool.
Equipment selection
Photobiomodulation LED panels are available in different sizes and powers. For targeted thyroid use, a small portable device (torch or pad format) with 660 nm and/or 850 nm LEDs is sufficient. The budget is 50 to 200 euros for a quality device. The essential criteria are wavelength (660 nm for red, 850 nm for near-infrared), power (30 to 50 mW/cm2 measured at the surface), and absence of flicker (flicker-free, some budget devices flicker at 50 Hz which can cause headaches).
For circadian light therapy, a certified 10,000 lux lamp at 30 cm, UV-free, from a recognized brand, costs between 50 and 150 euros. It is a worthwhile investment for any thyroid patient, especially in autumn and winter when natural light is insufficient.
The question of antioxidants
An important and counter-intuitive point: photobiomodulation works partly through the production of free radicals (ROS) that serve as cellular regeneration signals. If you take powerful antioxidants (NAC, high-dose vitamin C, reduced glutathione) in the hours before or after a red light session, you risk neutralizing these signals and reducing the effectiveness of the treatment.
The pragmatic solution is to space antioxidants two to three hours apart from the photobiomodulation session. Take supplements in the evening if the session is in the morning, or vice versa. It is not a major obstacle but it is a detail that can make the difference between an average result and an optimal one.
Cautions
Photobiomodulation is contraindicated directly over thyroid cancer (cellular stimulation could theoretically promote tumor proliferation). It is inadvisable in Graves’ disease (autoimmune hyperthyroidism) as thyroid stimulation could worsen hyperthyroidism. Patients on Levothyrox should have their panel monitored every two to three months as improved thyroid function may require dose reduction (otherwise risk of overdosing).
Morning light therapy is contraindicated in unstabilized bipolar disorder (risk of triggering a manic episode) and retinal pathology (macular degeneration, diabetic retinopathy). In these cases, consult an ophthalmologist before starting.
Salmanoff, who used light baths in his hydrotherapeutic practice, said that “light is a food in the same way as food and air. A body deprived of light is a sick body, as a body deprived of food is a starving body.” In our modern world of closed interiors, artificial lighting and screens, deficiency in natural light is perhaps the most universal and least recognized deficiency. Before seeking sophisticated supplements, start by going out in the morning and turning off screens in the evening. Light is free, and it may be the first medicine for your thyroid.
Want to assess your status? Take the free Claeys thyroid questionnaire in 2 minutes.
If you want personalized support, you can book a consultation.
To go further
- Graves’ disease and heart: calming the cardiac storm
- Graves’ disease and pregnancy: conceiving and carrying safely
- Graves’ disease and stress: the thyroid of emotion
- Sleeping well naturally: what naturopathy can offer you
Want to assess your status? Take the free Hertoghe melatonin questionnaire in 2 minutes.




Laisser un commentaire
Sois le premier à commenter cet article.