
Nathalie is fifty-two years old and has been taking omeprazole for seven years. Initially, it was for acid reflux after meals. Her doctor had diagnosed gastroesophageal reflux disease and prescribed a PPI “to calm the acidity.” Seven years later, Nathalie still has her reflux episodes (which she manages by increasing the dose), but she has developed chronic fatigue, hair loss, striated and brittle nails, ferritin at 12 ng/mL despite iron supplementation for two years, and B12 in the basement.
When I saw her in consultation, I requested a complete thyroid panel. TSH at 4.8 mIU/L (“normal” by lab standards, functionally elevated). Free T4 in the lower third. Low free T3. Anti-TPO at 145. A Hashimoto that no one had looked for. And urine iodine at 62 mcg/L. I also ordered a urea breath test: Helicobacter pylori positive.
Nathalie had three overlapping causes of hypochlorhydria: the hypothyroidism that was slowing down her parietal cells, Helicobacter pylori that was atrophying them, and omeprazole that was blocking the few remaining proton pumps. Her reflux had never been excess acid. It was a deficit. And the PPIs had made it worse for seven years.
Hydrochloric acid: much more than a solvent
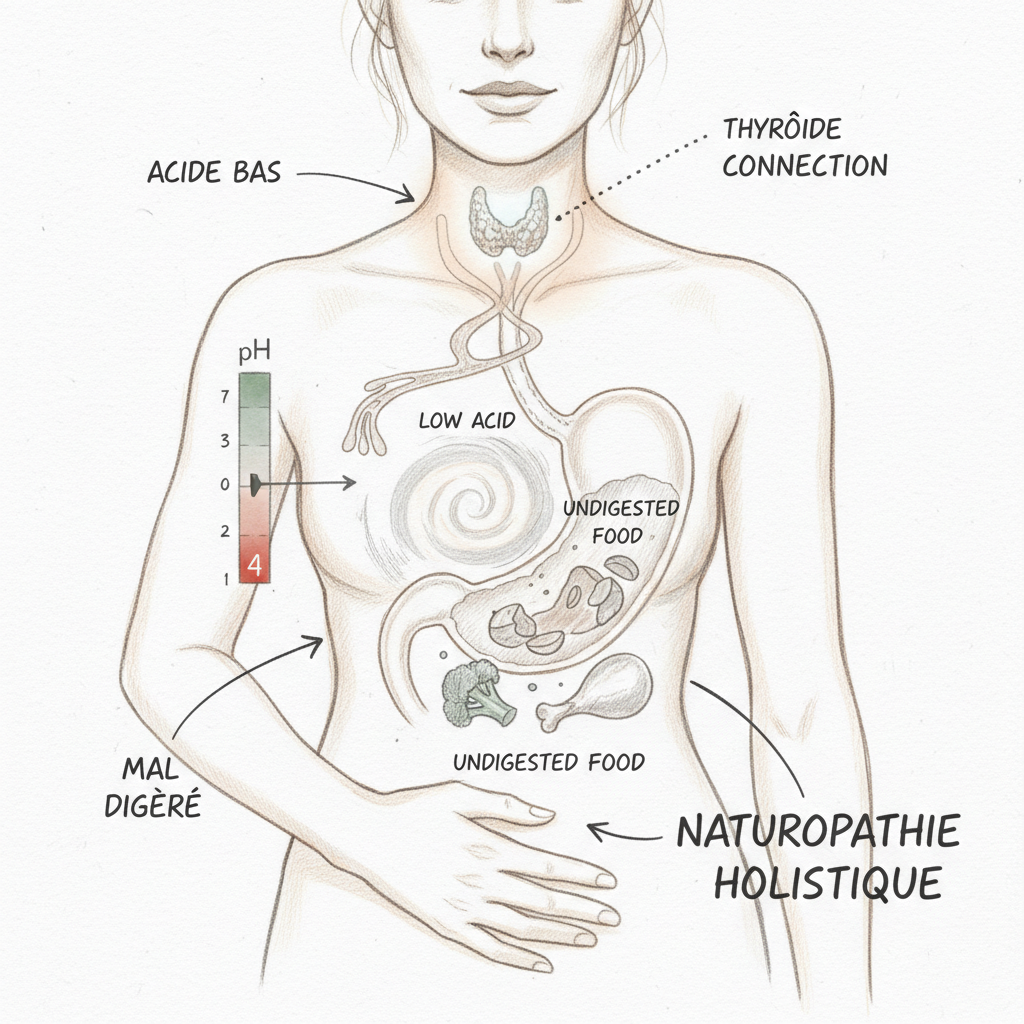
Gastric fluid has a pH between 1 and 3. It is one of the most acidic environments in the human body. This extreme acidity is not a design flaw. It is a biological necessity.
Hydrochloric acid (HCl) is produced by the parietal cells of the stomach through the H+/K+-ATPase proton pump. This pump consumes energy (ATP) to expel hydrogen ions (H+) into the gastric lumen against a colossal concentration gradient. It is one of the most energy-consuming reactions in the body. When the mitochondria of parietal cells are tired (hypothyroidism, iron deficiency, zinc deficiency), the pump slows down and acid production drops.
Acid performs five essential functions. The first is protein digestion: HCl activates pepsinogen into pepsin, the enzyme that breaks proteins into peptides and amino acids. Without sufficient acid, proteins are poorly digested in the small intestine where they ferment and cause bloating, foul-smelling gas, and local inflammation.
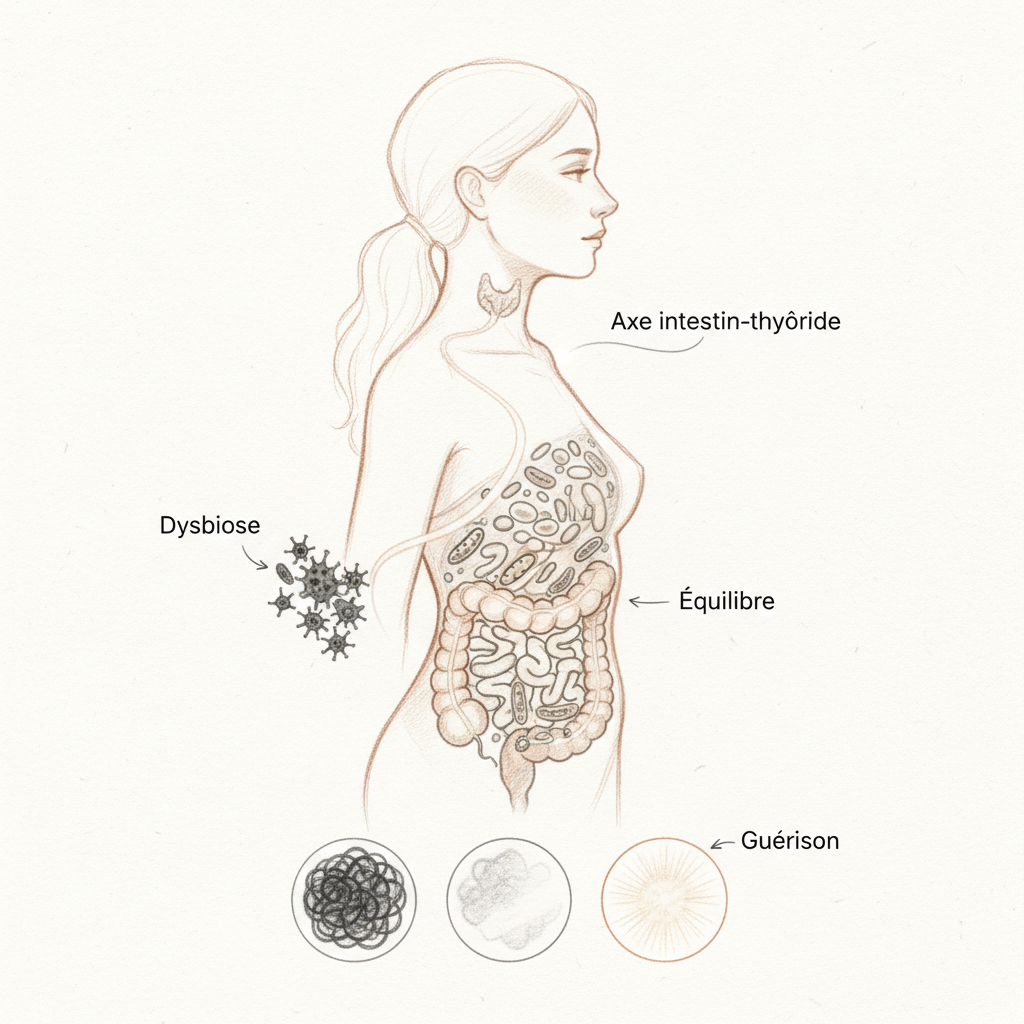
The second function is sterilization of the food bolus. Stomach acidity is the first antimicrobial barrier of the digestive tract. It kills most bacteria, yeasts, and parasites ingested with food. When this barrier fails (pH above 4), pathogens survive and colonize the small intestine. This is one of the main causes of SIBO (small intestinal bacterial overgrowth).
The third function is mineral absorption. Iron, zinc, calcium, magnesium, and chromium require an acidic environment to be ionized and absorbed. In hypochlorhydria, these minerals pass through the digestive tract without being assimilated. This is why so many hypothyroid patients have iron deficiencies resistant to supplementation: the iron is in the capsule, but the stomach cannot prepare it for absorption.
The fourth function is vitamin B12 absorption. Dietary B12 is bound to proteins. Gastric acid is necessary to release it, then intrinsic factor (also secreted by parietal cells) transports it to the terminal ileum for absorption. In hypochlorhydria, B12 remains trapped in food proteins and is never absorbed. B12 deficiencies in long-term PPI patients are well documented.
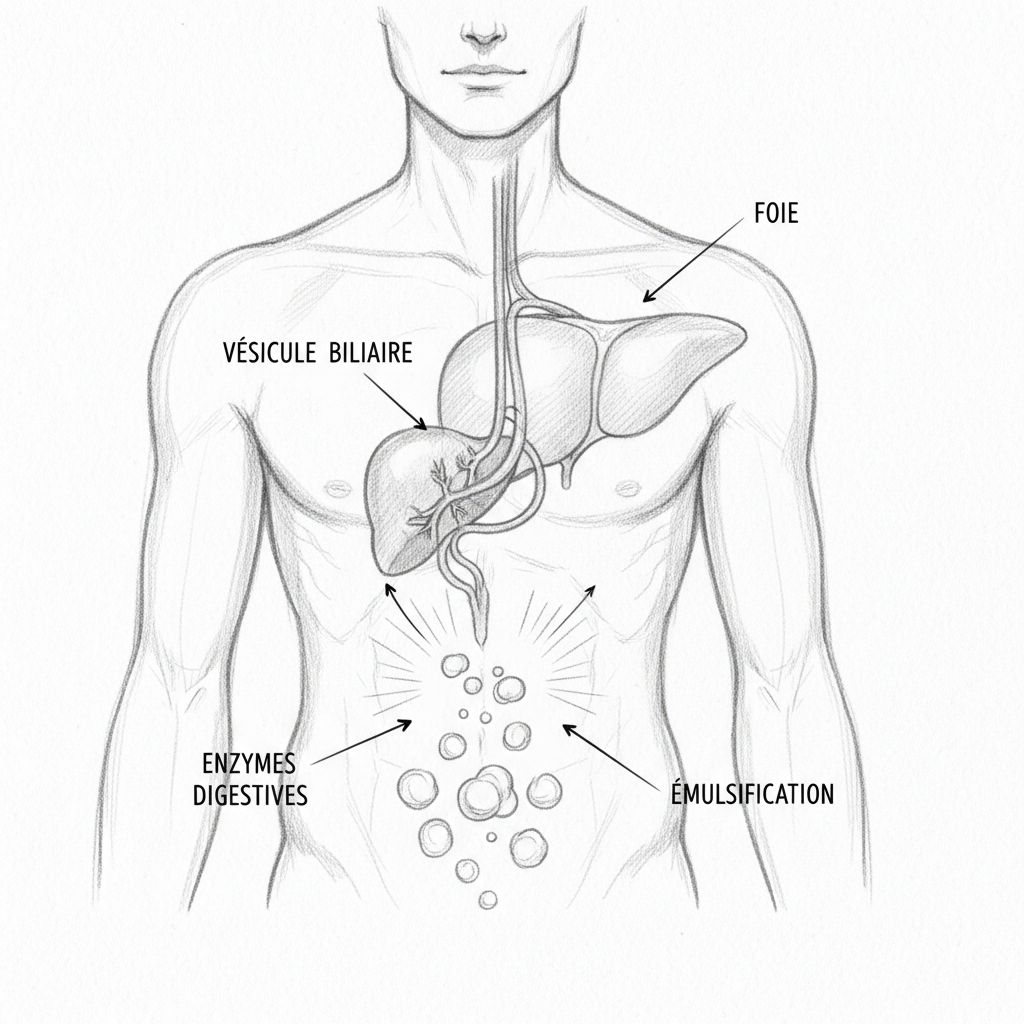
The fifth function is the downstream signal. Gastric acidity triggers the digestive cascade: it stimulates the secretion of secretin and cholecystokinin (CCK) by the duodenum, which in turn stimulate the secretion of bile and pancreatic enzymes. Without the initial acid signal, the entire downstream cascade runs slowly. This is why hypochlorhydria does not manifest only at the stomach level but disturbs the entire digestion.
The stomach trap: confusing deficit and excess
This is the most frequent trap I encounter in consultation. The patient has acid reflux, burning, a sensation of “too much acid.” The doctor prescribes a PPI. Symptoms improve temporarily (because less acid comes back up). The patient stays on PPI for years. And the underlying problem worsens silently.
Gastroesophageal reflux disease (GERD) is not excess acid. It is acid coming back up where it should not be. The lower esophageal sphincter, the muscle that closes the stomach entrance, contracts in response to the acidic pH of stomach contents. When acidity is insufficient, the sphincter does not close properly and contents come back up. It is a closure defect, not a production excess.
This paradox explains why so many PPI patients continue to have reflux: the medication reduces acid but does not correct the closure mechanism. And by reducing acid, it worsens the malabsorption that worsens hypothyroidism that worsens hypochlorhydria. The vicious cycle is perfect.
PPIs (omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole) are among the most prescribed medications in the world. They reduce gastric acid production by ninety percent. Initially designed for short-term treatments (ulcer, H. pylori eradication), they are prescribed long-term in millions of patients. Yet Finnish researchers showed that seven days of lansoprazole in healthy men is enough to raise gastric pH from 1.3 to 6.1, allowing bacterial colonization of the stomach and acetaldehyde production (carcinogenic) from ingested alcohol.
Mouton, in his treatise on digestive ecology, is categorical about PPIs: “Proton pump inhibitors are the most overused medications in modern medicine. They create the conditions for a silent digestive catastrophe: bacterial overgrowth, malabsorption, dysbiosis, immunosuppression. Their prescription should be limited to specific indications and short durations.”
The thyroid-stomach link
The relationship between thyroid and stomach is bidirectional and deeper than one might imagine.
In the thyroid-to-stomach direction, thyroid hormones (mainly T3) directly stimulate gastric parietal cells. They increase the expression of proton pumps, stimulate gastrin production (the hormone that commands acid secretion), and maintain vascularization of the gastric mucosa. In hypothyroidism, these three mechanisms fail. Acid production drops. This is why hypochlorhydria is found in the majority of untreated hypothyroid patients, and in many treated patients whose free T3 remains low despite “adequate” Levothyroxine dose.
In the stomach-to-thyroid direction, hypochlorhydria prevents the absorption of cofactors essential to thyroid function. Iron is necessary for thyroperoxidase (TPO), the enzyme that makes thyroid hormones. Zinc is a cofactor for hormone synthesis and cellular T3 reception. Selenium activates the deiodinase that converts inactive T4 to active T3. B12 is essential for methylation and cellular energy production. When these nutrients are not absorbed because of lack of acid, the thyroid slows down even more.
This vicious cycle is aggravated by a third player: autoimmunity. Hashimoto is the most frequent cause of hypothyroidism. Yet thyroid autoimmunity (anti-TPO, anti-thyroglobulin) is often associated with autoimmune gastritis (antibodies against parietal cells and intrinsic factor). Studies show that 20 to 40% of Hashimoto patients have anti-parietal cell antibodies. The same immune dysregulation that attacks the thyroid can also attack the stomach. This is the “autoimmune polyendocrinopathy” that Hertoghe describes as an under-diagnosed phenomenon.
Helicobacter pylori: the silent enemy
Helicobacter pylori infects half the world’s population. In France, prevalence is approximately 20 to 30% in adults. This spiral bacterium has a unique capacity: to survive and thrive in stomach acid thanks to urease production, an enzyme that transforms urea into ammonia, creating an alkaline micro-environment around the bacterium.
But H. pylori does not just neutralize acid locally. It causes chronic gastritis that progressively atrophies parietal cells. It blocks existing proton pumps and reduces the expression of the gene that codes for them, decreasing their total number. The result is chronic hypochlorhydria that worsens over years of infection.
The relationship between H. pylori and the thyroid is bidirectional. On one hand, hypochlorhydria caused by H. pylori worsens hypothyroidism through malabsorption. On the other, hypothyroidism reduces gastric motility and local immunity, creating an environment favorable to H. pylori persistence. Several studies show that H. pylori eradication improves Levothyroxine absorption and may allow dose reduction in thyroid patients.
H. pylori screening should be systematic in any hypothyroid patient presenting upper digestive symptoms (burning, reflux, post-meal heaviness, belching). The carbon 13 urea breath test is non-invasive and reliable. Eradication typically relies on triple antibiotic therapy, but complementary approaches exist: Chios mastic (resin from Pistacia lentiscus, 500 mg three times daily for two weeks), sulforaphane (sprouted broccoli extract, which inhibits H. pylori in vitro), and NAC (N-acetylcysteine, which destroys H. pylori biofilm and improves antibiotic effectiveness).
The protocol in practice
The first step is diagnosis. Above all, hypochlorhydria must be confirmed and its cause identified. The baking soda test is a first home indicator: on an empty stomach in the morning, dissolve half a teaspoon of sodium bicarbonate in a glass of water, drink it in one go, and time the first belch. Less than two minutes: acidity probably adequate. Two to five minutes: acidity probably insufficient. More than five minutes or no belch: hypochlorhydria very likely. This test is not a medical diagnosis but it provides direction.
The apple cider vinegar test completes the picture: one teaspoon of apple cider vinegar in half a glass of water before a meal. If digestive symptoms improve (less heaviness, less bloating), it means the stomach lacked acid. If symptoms worsen (burning), acidity is probably sufficient or a mucosal lesion is present. These two tests are described in detail in the stomach pH questionnaire on the site.
The second step is treating the cause. If H. pylori is positive, eradication is the priority. If PPIs are ongoing, gradual withdrawal is essential (reduce dose by half for two weeks, then quarter dose for two weeks, then stop, accompanied by natural alternatives below). If hypothyroidism is identified, thyroid treatment (Levothyroxine or natural thyroid) will gradually improve acid production in four to eight weeks. Consult the article on the 7 thyroid nutrients for essential cofactors.
The third step is natural acid support. Apple cider vinegar (one teaspoon in half a glass of water, fifteen minutes before each main meal) is the simplest gesture and often the most effective. Fresh ginger (a two-centimeter slice infused ten minutes in hot water, drunk before the meal) stimulates gastric motility and acid secretion. Bitter herbs (gentian, artichoke, dandelion) in mother tincture (thirty drops in a little water ten minutes before the meal) activate the digestive cascade through the bitter cephalic reflex.
The fourth step is betaine HCl (under professional supervision). This supplement directly provides hydrochloric acid to the stomach. The titration protocol consists of taking one 500 mg capsule in the middle of a meal containing animal protein (meat, fish, eggs). If no sensation of warmth or burning appears, increase by one capsule at the next meal. Continue increasing by one capsule per meal until feeling slight gastric warmth, then reduce by one capsule. This dose is the maintenance dose. It can vary from 500 mg to 3000 mg depending on hypochlorhydria severity. Betaine HCl is strictly contraindicated in case of active ulcer, erosive gastritis, NSAIDs or corticosteroid use.
The fifth step is correcting secondary deficiencies. Hypochlorhydria creates deficiencies in iron, zinc, B12, magnesium, and calcium that must be corrected in parallel. But beware: supplementing without correcting gastric acidity is throwing supplements down the drain. The priority is restoring absorption before loading up on micronutrients. Chelated forms (iron bisglycinate, zinc bisglycinate, magnesium citrate) are better absorbed in low-acid environments than oxide or sulfate forms. B12 in sublingual methylcobalamine form bypasses the gastric problem by being absorbed directly through the oral mucosa.
The sixth step is protecting and regenerating the mucosa. Hypertonic quinton water (one ampoule before the meal) provides marine trace elements and stimulates gastric secretion. Glutamine (four grams per day) nourishes the intestinal mucosal cells. Zinc-carnosine (75 mg twice daily) is specifically protective of the gastric mucosa and has shown effectiveness in repairing lesions caused by H. pylori and NSAIDs.
Eating to support acidity
Animal proteins are the most powerful natural stimulators of acid secretion. They work in two ways: by stimulating gastrin production (the hormone that commands HCl secretion) and by directly stimulating parietal cells via absorbed amino acids. This is probably why many people with chronic hypochlorhydria feel improvement with a diet rich in quality animal protein (eggs, fish, white meat).
Bone broth is a valuable ally. Rich in glycine, proline, and glutamine, it nourishes the gastric mucosa while providing minerals in bioavailable form. A bowl of warm broth fifteen minutes before the meal prepares the stomach for digestion.
Fermented foods (raw sauerkraut, kimchi, kefir, kombucha) provide organic acids and enzymes that support digestion. Their acidic pH helps maintain a favorable gastric environment. However, they should be introduced gradually in SIBO patients (fermentation can worsen bloating).
Methylxanthines (coffee, tea, chocolate) stimulate acid secretion but irritate the mucosa and relax the lower esophageal sphincter. In the presence of reflux, they should be avoided despite their stimulating effect on acid. This is a trade-off to evaluate individually.
PPI withdrawal
Stopping PPIs after years of use does not happen overnight. The rebound acid hypersecretion phenomenon is well documented: when proton pumps are unblocked after months of suppression, they temporarily overproduce acid, causing intense burning that pushes the patient to resume the medication. This rebound lasts two to four weeks.
Gradual withdrawal protocol is essential. Reduce dose by half for two weeks. Then take half a tablet every other day for two weeks. Then stop. Throughout withdrawal, accompany with apple cider vinegar before meals, melatonin in the evening (three milligrams, which has shown a protective effect against reflux comparable to PPIs in some studies), baking soda as needed (a knife tip in a glass of water in case of acute burning, occasionally), and anti-reflux herbs (marshmallow, DGL licorice, aloe vera).
Kousmine, in her orthomolecular medicine approach, emphasized that “suppressing a symptom without seeking its cause is turning off the alarm without extinguishing the fire. Anti-acids are the perfect example of medicine of silence. They turn off pain but feed disease.”
Warnings
Hypochlorhydria is a symptom, not a diagnosis. It can be caused by hypothyroidism, H. pylori, PPIs, autoimmune gastritis, aging, chronic stress, zinc deficiency, or a combination of these factors. Identifying the cause is essential before treating.
Betaine HCl is formally contraindicated in case of gastric or duodenal ulcer, erosive gastritis, anti-inflammatory use (NSAIDs, aspirin), or corticosteroids. Any acute stomach pain, any vomiting of blood, or any black stools (melena) requires urgent medical consultation and gastroscopy.
PPI withdrawal must be gradual and supported. Abrupt discontinuation can cause severe acid rebound. If PPIs were prescribed for a documented ulcer or Barrett’s esophagus, withdrawal only occurs with gastroenterologist approval.
Masson, in his food philosophy, reminded us that “the stomach is the body’s first laboratory. When it works poorly, everything that follows is compromised. Before seeking sophisticated solutions downstream, verify that the upper level is doing its job.” Nathalie, who was able to stop her PPIs after seven years and recover normal ferritin in six months of thyroid correction and gastric support, would confirm. If you want personalized support, you can book a consultation.
To go further
- Bloating and gas: your belly is trying to talk to you
- Bile and gallbladder: the forgotten key to your digestion
- Chronic constipation: the 7 causes your doctor is not looking for
- Chronic diarrhea: the deep causes no one is looking for
Want to assess your status? Take the free Claeys thyroid questionnaire in 2 minutes.



Laisser un commentaire
Sois le premier à commenter cet article.