
Samir is forty-five years old, diagnosed with Hashimoto’s at thirty-eight, with anti-TPO antibodies that won’t drop below 400 despite three years of rigorous naturopathic protocol. Gluten-free for three years. Dairy-free for two years. Selenium 200 micrograms daily. Zinc 30 mg. Optimal vitamin D. Intestines treated (SIBO eradicated, permeability restored). Stress managed (heart coherence, meditation, proper sleep). Liver supported (castor oil poultice twice weekly). Everything is in place. But the antibodies are stagnant.
I asked the question I systematically ask when a patient is doing “everything right” but not progressing: “What about your mouth?” Samir looked at me without understanding. His mouth? What does that have to do with his thyroid?
He came back two weeks later with a complete dental assessment. Moderate chronic periodontitis (pockets of 4 to 6 mm on several molars). Three mercury amalgams, one of them cracked. And an infected root canal tooth under crown for eight years (apical granuloma visible on panoramic X-ray).
Six months after intensive periodontal treatment, secure amalgam removal (SMART protocol), and extraction of the infected tooth, his anti-TPO had dropped from 420 to 185. The most dramatic drop in his entire journey. The mouth was the silent infectious focus that had been fueling autoimmunity for years.
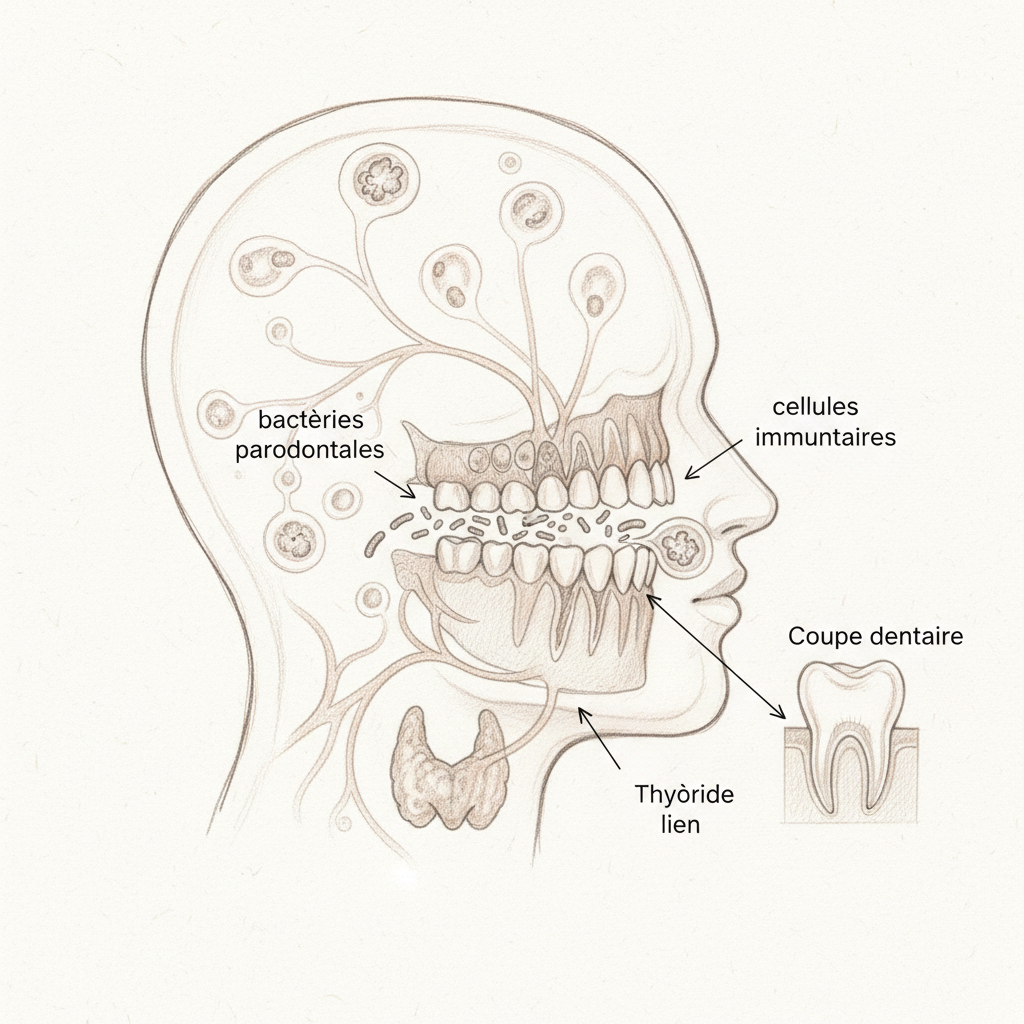
The mouth: gateway to systemic inflammation
The oral cavity hosts more than 700 different bacterial species. It’s the second most diverse microbiome in the human body after the intestine. In good health, these bacteria live in symbiotic balance with the host. But when hygiene is insufficient, when diet is unbalanced (excess sugar), when the immune system is weakened, or when local factors disrupt the balance (amalgams, poorly fitted crowns, root canal teeth), pathogenic bacteria take over and cause chronic inflammation.
Periodontitis is the most common expression of this imbalance. It affects 50% of adults over thirty to varying degrees, and 10 to 15% severely. It’s an insidious disease, often painless for years, which progressively destroys the alveolar bone that supports teeth. But its consequences far exceed the mouth.
Porphyromonas gingivalis, the key bacterium in periodontitis, produces enzymes (gingipains) that destroy tissues and endotoxins (lipopolysaccharides/LPS) that enter the bloodstream with every tooth brushing, chewing, and dental treatment. These LPS activate the innate immune system (via TLR4 receptors), trigger production of pro-inflammatory cytokines (TNF-alpha, IL-1, IL-6), and maintain chronic low-grade systemic inflammation.
Kousmine, in the 1980s, already emphasized dental infectious foci as causes of autoimmune and degenerative diseases. She wrote: “A chronic dental focus is like a toxin factory operating day and night, pouring its poisons into the blood and keeping the immune system in a state of permanent alert.”
Periodontitis and thyroid: the autoimmune link
Several epidemiological studies show a significant association between periodontitis and autoimmune thyroid disease. Hashimoto’s patients have significantly higher prevalence of periodontitis than controls. And conversely, patients with severe periodontitis have increased risk of developing autoimmune thyroiditis.
The most likely mechanism is molecular mimicry. Certain P. gingivalis proteins have amino acid sequences similar to thyroid proteins (notably thyroglobulin and TPO). The immune system, in producing antibodies against bacterial proteins, creates antibodies that also recognize (by mistake) thyroid proteins. It’s the same mechanism linking gluten and Hashimoto’s: wheat gliadin resembles thyroid transglutaminase, and anti-gliadin antibodies also attack the thyroid.
The other mechanism is non-specific immune activation. Chronic periodontal inflammation keeps the immune system in a state of permanent hyperactivity. In this state, targeting errors (autoimmunity) are more frequent. It’s like an overly sensitive alarm system that keeps triggering without reason: the immune system, constantly overstimulated by oral bacteria, ends up attacking the body’s own tissues.
Mercury amalgams: the silent disruptor
Dental amalgams (gray “fillings”) contain approximately 50% mercury, 35% silver, and 15% tin and copper. Mercury is released continuously as vapor, in amounts increased by chewing, brushing, teeth grinding (bruxism), hot beverages, and acidic foods. This vapor is inhaled, absorbed by oral mucous membranes, and enters the bloodstream.
Mercury has particular affinity for organs rich in selenium (because it binds to selenium to form mercury selenide, an inert compound). Now the thyroid is the organ richest in selenium in the human body (selenium is the cofactor of deiodinases that convert T4 to T3). Mercury from amalgams therefore concentrates preferentially in the thyroid, where it inhibits deiodinases, blocks T4 to T3 conversion, and can trigger an autoimmune response.
Studies show that amalgam removal is followed by improvement in thyroid parameters in Hashimoto’s patients, with a drop in antibodies and sometimes TSH normalization. But removal must be done according to the SMART protocol (Safe Mercury Amalgam Removal Technique) which includes: rubber dam to isolate the tooth, high-volume suction, nasal mask with oxygen or filtered air supply, removal in large chunks (no spraying), and activated charcoal before and after for the patient. Removal without precaution exposes the patient to a massive dose of mercury vapor that can acutely worsen autoimmunity.
Root canal teeth: hidden infectious foci
A root canal tooth (having undergone endodontic treatment) is a tooth whose nerve has been removed and channels filled with filling material. In theory, the tooth is “sterile.” In practice, accessory channels (there are dozens per tooth, invisible on X-ray) remain colonized by anaerobic bacteria that continuously produce toxins.
These toxins (thiethers, mercaptans) are endocrine disruptors and immunotoxins. They enter the bloodstream via the alveolar bone and maintain low-grade chronic inflammation. The apical granuloma (small infection at the tip of the root, visible on panoramic X-ray or cone-beam) is the most common manifestation of this chronic infectious focus.
Conventional dentistry considers most root canal teeth “healthy” as long as there’s no pain or visible infection. Holistic (or biological) dentistry is more cautious and proposes either thorough endodontic retreatment (with bioceramic obturation rather than gutta-percha), or extraction followed by bone curettage and implantation or bridging.
The six-point oral health audit
The first point is the periodontal assessment. Ask your dentist for complete periodontal probing (pocket depth measurement). Any pocket greater than 3 mm should be treated (subgingival scaling, root planing, possibly local antibiotic therapy).
The second point is the amalgam inventory. Count the number of amalgams, note their condition (cracked, worn, corroded). Plan progressive removal by a dentist trained in the SMART protocol. One amalgam per session, starting with the most damaged ones, with four to six weeks of recovery between each removal.
The third point is the root canal tooth assessment. Ask for a panoramic X-ray (or cone-beam for greater precision) to identify apical granulomas. Discuss with a holistic dentist the opportunity for retreatment or extraction.
The fourth point is switching from fluoridated toothpaste. Fluorine is a halogen that displaces iodine in the thyroid. Switch to hydroxyapatite toothpaste (remineralizing without fluorine) or white clay.
The fifth point is introducing oil pulling. One tablespoon of virgin coconut oil, to be circulated in the mouth for fifteen to twenty minutes each morning on an empty stomach, then spit out (don’t swallow). The lauric acid in coconut oil has documented antimicrobial properties against P. gingivalis and Streptococcus mutans.
The sixth point is periodontal nutrition. Vitamin C (citrus, kiwi, bell pepper) is essential for gingival collagen synthesis. Coenzyme Q10 (200 mg daily) reduces periodontal inflammation and pocket depth. Zinc (30 mg daily) supports mucosal immunity. Vitamin D (optimize to 40-60 ng/mL) modulates inflammation and bone remodeling. Omega-3s (EPA/DHA 2 g daily) reduce pro-inflammatory cytokines.
The support protocol during amalgam removal
The pre-removal phase (two weeks before) consists of saturating selenium reserves (200 mcg daily), NAC/glutathione (NAC 600 mg twice daily), vitamin C (2 g daily), and chlorella (3 g daily). These nutrients prepare mercury detox pathways.
Day of removal: activated charcoal 2 g two hours before and two hours after the appointment. Chlorella 3 g after the appointment. Drink plenty of water.
The post-removal phase (four to six weeks) maintains the gentle chelation protocol: chlorella 3 g daily (which binds mercury in the intestine), fresh cilantro (which mobilizes mercury from tissues, to be used ONLY with a binder like chlorella), NAC 600 mg twice daily, selenium 200 mcg, and infrared sauna three times weekly to eliminate mercury through sweat.
Warning
Amalgam removal without precaution can cause acute mercury poisoning (headaches, severe fatigue, brain fog, worsening autoimmune symptoms). NEVER have an amalgam removed by a dentist unfamiliar with the SMART protocol. Better to keep an intact amalgam than have it removed dangerously.
Pregnant or nursing women must NOT have their amalgams removed (mobilized mercury crosses the placental barrier and enters breast milk). Wait until breastfeeding is finished.
Extraction of a root canal tooth is an important decision that should be made case by case, in collaboration with a dentist and naturopath. Not all root canal teeth are infectious foci and systematic extraction is not justified.
Marchesseau taught that “toxemia is the cause of all diseases.” Dental infectious foci are a source of chronic toxemia that modern naturopathy tends to neglect in favor of the intestine and liver. Yet the mouth is the first entry point of the digestive tract, and what enters the mouth conditions everything that happens downstream. A complete thyroid assessment without an oral health audit is an incomplete assessment.
Want to evaluate your status? Take the free Claeys thyroid questionnaire in 2 minutes.
If you want personalized support, you can schedule a consultation.




Laisser un commentaire
Sois le premier à commenter cet article.