Sandrine is forty-one years old and has breast pain fifteen days a month. Not a mild discomfort but frank, throbbing pain that radiates to her armpits and prevents her from sleeping on her stomach. Both breasts are “lumpy” (her word) with hard areas that vary in size depending on where she is in her cycle. Her gynecologist told her it was “benign fibrocystic mastopathy,” prescribed Progestogel (progesterone in local gel form) and advised her to limit coffee. The pain did not decrease.
When Sandrine came in for consultation, I noted in her assessment: TSH at 3.6 mIU/L (“normal” according to the lab but functionally elevated), anti-TPO at 95 (an early Hashimoto that no one had looked for), an estradiol/progesterone ratio showing frank estrogen dominance in the luteal phase, and iodine excretion at 52 mcg/L (moderate deficiency, WHO norm being above 100 mcg/L). She was drinking four coffees a day.
Sandrine had the perfect triangle: sluggish thyroid, iodine deficiency and estrogen dominance. Three months after correction (stopping coffee, selenium + myo-inositol for thyroid, DIM for estrogens, careful iodine supplementation under monitoring), her breast pain had decreased by 70%. At six months, she could sleep on her stomach again. Her breasts were no longer “lumpy.” And her TSH had dropped to 2.1.
Iodine: not just for the thyroid
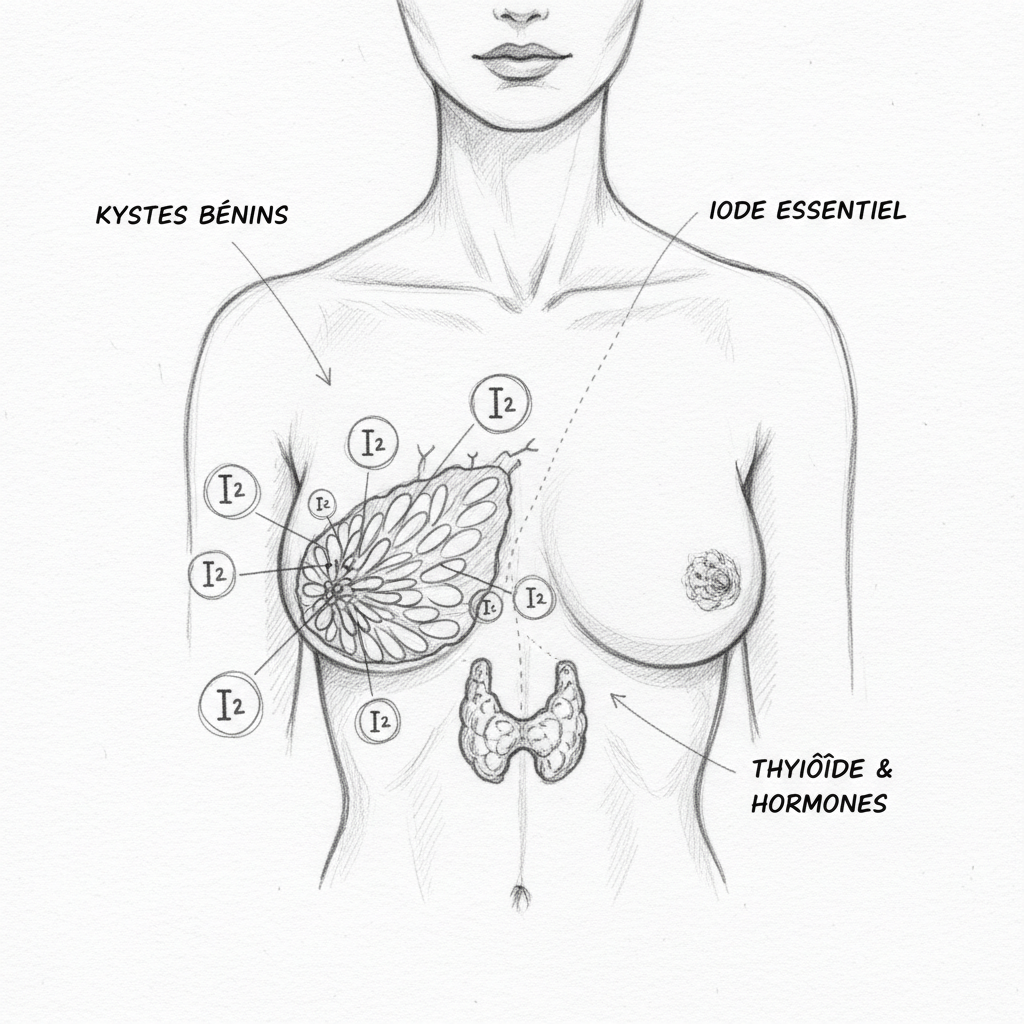
When we talk about iodine, we immediately think of the thyroid. That’s normal: the thyroid concentrates iodine through the sodium-iodide symporter (NIS) to make T3 and T4 hormones. But NIS is not exclusive to the thyroid. It is also found in the breasts (breast tissue), ovaries, stomach, salivary glands and the choroid plexus of the brain. These tissues actively concentrate iodine and need it for normal functioning.
In breast tissue, iodine plays a major anti-proliferative role. It induces apoptosis (programmed cell death) of abnormal cells, inhibits excessive cell proliferation and reduces local inflammation. These functions are essential for maintaining normal breast architecture and preventing cyst formation and fibrosis.
When iodine is insufficient (and it is in 30 to 40% of French women), breast cells proliferate in a disorderly manner, milk ducts dilate and fill with fluid (cysts), and connective tissue fibroses. This is fibrocystic mastopathy, which affects 60% of women of childbearing age and is considered by conventional medicine to be a “variant of normal.”
Curtay, in his nutritherapy approach, contests this trivialization: “To say that a condition affecting 60% of women is normal is to confuse frequency with normalcy. Dental cavities also affect the majority of the population. That doesn’t make them normal. Fibrocystic mastopathy is a sign of nutritional and hormonal imbalance that deserves to be corrected, not trivialized.”
The breast-thyroid-estrogen triangle
The link between fibrocystic breasts and thyroid is threefold.
The first link is iodine. Iodine deficiency affects both the thyroid (hypothyroidism) and the breasts (fibrocystic mastopathy). Epidemiological studies show that countries with high iodine consumption (Japan, Korea) have a much lower incidence of fibrocystic mastopathy and breast cancer than countries with low iodine consumption (Western Europe). Average iodine consumption in Japan is 5 to 13 mg per day (mainly from seaweed), compared to 100 to 150 mcg in France. That’s 50 to 100 times more.
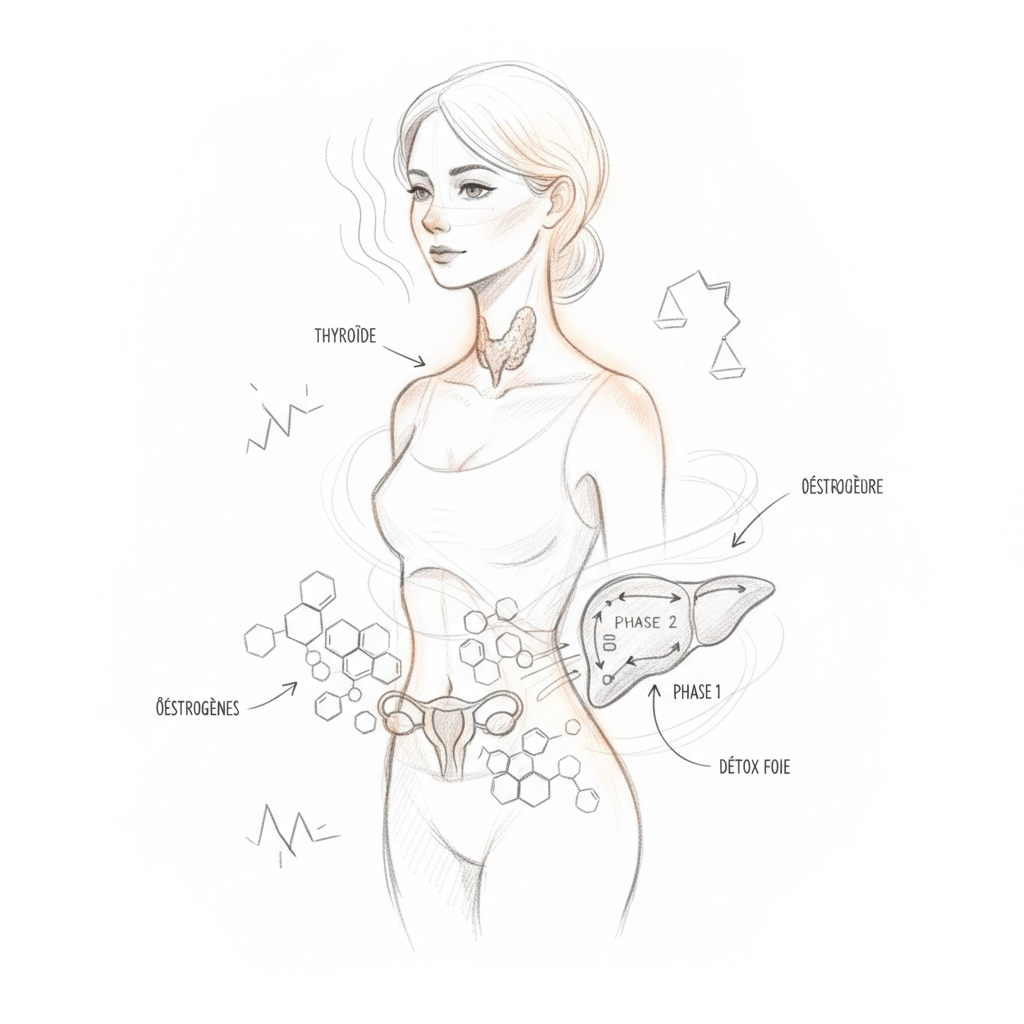
The second link is estrogen. Estrogens stimulate cell proliferation in the breasts (which is why breasts swell in the premenstrual phase and during pregnancy). In estrogen dominance (excess estrogen relative to progesterone), this stimulation is chronic and excessive, promoting cyst formation and fibrosis. Estrogen dominance is common in hypothyroid women: hypothyroidism slows the liver’s metabolism of estrogens, which accumulate instead of being eliminated. And excess estrogens increase TBG, which reduces free thyroid hormones and worsens hypothyroidism. It’s a vicious cycle.
The third link is progesterone. Progesterone is the natural antagonist of estrogen in the breasts: it slows cell proliferation and promotes differentiation. In hypothyroidism, progesterone production is often insufficient (hypothyroidism disrupts ovulation and formation of the corpus luteum). And in perimenopause, the drop in progesterone precedes the drop in estrogens by several years, creating a window of estrogen dominance that corresponds exactly to the peak incidence of fibrocystic mastopathy.
Molecular iodine: the therapeutic approach
Three forms of iodine exist: potassium iodide (KI, the form in standard supplements and iodized salt), Lugol’s iodine (a mixture of iodide and molecular iodine) and molecular iodine (I2, the elemental form). These three forms are not interchangeable.
Iodide (I-) is preferentially taken up by the thyroid. Molecular iodine (I2) is preferentially taken up by the breasts and stomach. Clinical studies have shown that molecular iodine at a dose of 3 to 6 mg per day (in the form of diiodolipid or aqueous solution) significantly reduces breast pain and nodularity in 65 to 74% of women, with an onset of action of three to six months.
The advantage of molecular iodine is that it acts preferentially on the breasts without overloading the thyroid with iodide (which is important in Hashimoto patients where excess iodide can worsen autoimmunity). However, this form is difficult to find in France and iodine supplementation remains a controversial topic requiring professional monitoring.
The protocol in practice
The first step is stopping methylxanthines. Completely eliminate coffee, black tea, chocolate and colas for three months. This is often the most effective and fastest measure (improvement in four to six weeks). After three months without pain, gradually reintroduce to find individual tolerance threshold.
The second step is correcting estrogen dominance. DIM (diindolylmethane) 100 to 200 mg per day to improve liver metabolism of estrogens (promotes protective 2-OH pathway). Calcium D-glucarate 500 mg twice daily to inhibit intestinal beta-glucuronidase (which reabsorbs conjugated estrogens). Ground flax seeds (2 tablespoons per day) for their anti-estrogenic effect through lignans. Liver support (milk thistle, castor oil compress) to improve estrogen detoxification.
The third step is thyroid support. Selenium 200 mcg per day (cofactor of TPO and deiodinase). Myo-inositol 600 mg per day (improves TSH sensitivity). Zinc 30 mg per day (cofactor of hormone synthesis). Vitamin D 4000 IU per day (modulates autoimmunity). Complete thyroid assessment with follow-up every three months.
The fourth step is iodine supplementation (under supervision). Start with food sources: seaweed (wakame, nori, dulse) two to three times per week, saltwater fish, shellfish. If iodine excretion remains low despite diet, careful supplementation can be considered: 150 to 300 mcg of potassium iodide per day as a starting point, with monitoring of iodine excretion and thyroid antibodies at three months. Any dose increase must be gradual and supervised.
The fifth step is local support. Evening primrose oil 1000 to 2000 mg per day (gamma-linolenic acid, precursor of anti-inflammatory PGE1 prostaglandins). Vitamin E 400 IU per day (reduces breast sensitivity to estrogen). Local application of castor oil to the breasts (in light compress form, not on nipples) for local lymphatic drainage.
The link with breast cancer
Fibrocystic mastopathy is not a precancerous condition in itself. However, some histological types (atypical hyperplasia) moderately increase the risk of breast cancer. And the factors that maintain mastopathy (estrogen dominance, iodine deficiency, hypothyroidism) are the same ones that increase breast cancer risk.
The most striking ecological study is the Japan/West comparison. Japanese women, who consume 25 to 50 times more iodine than Western women (mainly through seaweed), have three to four times lower breast cancer incidence. When Japanese women emigrate to the United States and adopt a Western diet low in iodine, their breast cancer risk matches that of American women within one to two generations. This observation does not prove a direct causal link but it is consistent with the protective role of iodine in breast tissue.
Warning
Any new breast mass that is hard, fixed, painless or does not vary with the cycle must be evaluated by a doctor (mammography and/or ultrasound) BEFORE starting a naturopathic protocol. Fibrocystic mastopathy is a diagnosis of exclusion: cancer must be ruled out first.
Iodine supplementation in Hashimoto patients is a delicate matter. Excess iodine can worsen thyroid autoimmunity by increasing hydrogen peroxide production in the gland (iodine is oxidized by TPO, and this reaction produces H2O2 which, in excess, damages thyroid cells). Any iodine supplementation above 150 mcg per day in a Hashimoto patient must be accompanied by selenium (200 mcg, to support glutathione peroxidase which neutralizes H2O2) and monitored by anti-TPO antibody testing every three months.
Masson, in his philosophy of nutrition, recalled that “the most powerful nutrients are also the most dangerous when misused. Iodine heals the thyroid and breasts in adapted quantity. It damages them in excess. The dose makes the remedy and the poison.” This is why the naturopathic approach to iodine is always progressive, measured and accompanied by protective cofactors. Sandrine, who simply needed a little more iodine and a little less coffee, can testify to this.
Want to evaluate your status? Take the free Claeys thyroid questionnaire in 2 minutes.
If you want personalized support, you can book a consultation appointment.
To go further
- Estrogen dominance: when your hormones trap your thyroid
- Perimenopause and thyroid: the natural hormone protocol
- Thyroid and female hormones: the knot no one unties
- Graves’ disease and heart: calming the cardiac storm
Want to evaluate your status? Take the free Hertoghe estrogen questionnaire in 2 minutes.



Laisser un commentaire
Sois le premier à commenter cet article.