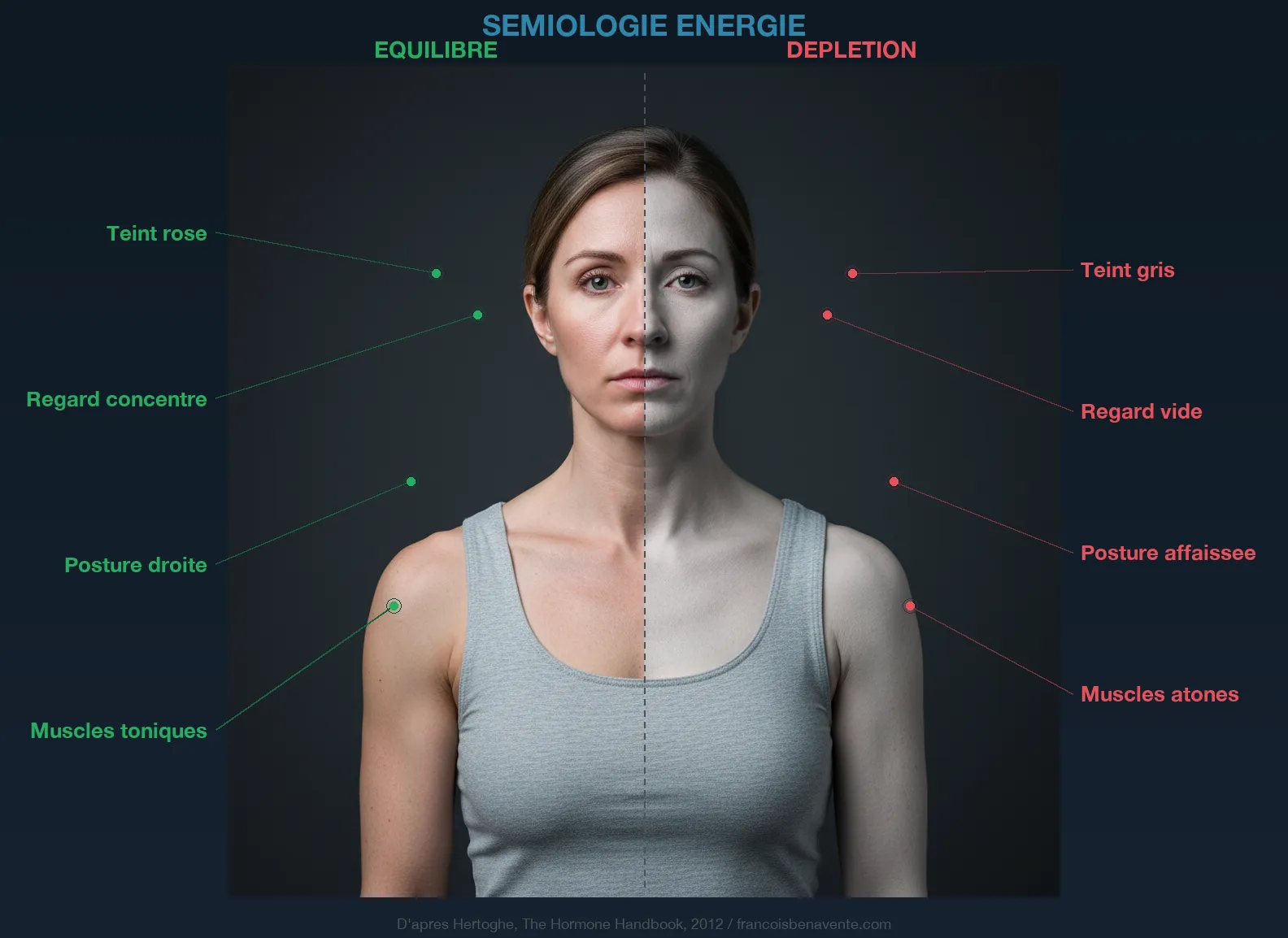
Isabelle is Fifty-two Years Old
Isabelle is fifty-two years old. She takes her Levothyrox every morning with the discipline of a Swiss clock, for six years now. Her TSH is at 1.8, her free T4 is correct, her endocrinologist is satisfied. And yet, every afternoon around two o’clock, she collapses. Not ordinary fatigue. A wall. An impossibility of continuing to think clearly, to concentrate, to remain standing. In the evening, she falls asleep on the couch at eight-thirty, but wakes at three in the morning with her brain churning and legs as heavy as lead. Her doctor told her everything was fine, since the numbers were good. He suggested an antidepressant. She refused. She felt it wasn’t in her head.
When I asked what she was eating, she described a strict vegetarian diet for the past four years. Little meat, no red meat, lots of whole grains and legumes. A diet that many would consider exemplary. But when I had her plasma carnitine level measured, the figure came back: 18 micromoles per liter, with a low normal of 25. Her mitochondria were running on empty. And no one had ever discussed this with her.
Carnitine is probably the most underestimated molecule in all thyroid micronutrition. It is neither a vitamin nor a mineral. It is a derived amino acid, synthesized by the liver and kidneys from two essential amino acids, lysine and methionine, with the help of four indispensable cofactors: vitamin C, iron, vitamin B6 and vitamin B3. Its role is simple to understand but fundamental: it transports long-chain fatty acids across the inner mitochondrial membrane so they can be burned there by beta-oxidation and transformed into ATP, the energy currency of each of your cells.
Without carnitine, no transport. Without transport, no combustion. Without combustion, no energy. And without energy, you collapse.
The Shuttle That Powers Your Power Plants
To understand carnitine’s role, you must first understand the mitochondrion. Each of your cells contains between a few hundred and several thousand mitochondria, those organelles that biology textbooks call the “power plants.” In your muscle cells, there are between one thousand and two thousand. In heart cells, up to five thousand. They’re there for one precise job: to transform energy substrates (glucose, fatty acids, amino acids) into ATP, adenosine triphosphate, which powers absolutely all the functions of your body.

Long-chain fatty acids, those that come from your fat reserves or your diet, are a substantial source of energy. Gram for gram, a fatty acid provides twice as much ATP as glucose. But there’s a problem: these molecules are too large to cross the inner mitochondrial membrane on their own. They remain blocked at the door, like a truck too wide to fit under a tunnel. And this is where carnitine comes in.
The mechanism is elegant. On the outer face of the mitochondrial membrane, an enzyme called CPT-I (carnitine palmitoyltransferase I) detaches the CoA group from the fatty acid and replaces it with a carnitine molecule. The acyl-carnitine complex thus formed is compact enough to cross the membrane through a specific transporter, the translocase. On the other side, a second enzyme (CPT-II) detaches the carnitine and reattaches the CoA. The fatty acid, finally inside the mitochondrion, can enter the beta-oxidation spiral and be split into two-carbon units that feed the Krebs cycle. Carnitine itself crosses back through the membrane in the opposite direction to fetch another fatty acid. It’s a shuttle. A tireless transporter that makes the connection between the cytoplasm and the interior of the mitochondrion, back and forth, thousands of times a day.
When this shuttle breaks down, fatty acids accumulate outside the mitochondrion without being burned. The cell then falls back on glucose as its main fuel, which causes blood sugar fluctuations, cravings, sugar dependence, and an inability to mobilize fat reserves. It’s like having a fireplace full of logs but no matches: the fuel is there, but it won’t burn. I addressed this inability to burn fats in my article about thyroid and weight, and carnitine is a cornerstone of it.
When Hypothyroidism Drains Your Reserves
This is where the thyroid enters the scene. T3, the active thyroid hormone, directly stimulates the expression of genes that code for beta-oxidation enzymes and carnitine transporters. When T3 is low, these enzymes slow down, the demand for carnitine increases (the system compensates by trying to force transport) and supplies become depleted. Studies of thyroid myopathy have shown that muscle carnitine reserves are significantly lowered in hypothyroid patients. It’s no accident that muscle fatigue is one of the first symptoms of hypothyroidism.
But the story doesn’t stop at fatigue. A remarkable study showed that L-carnitine supplementation in hypothyroid patients on Levothyrox increased peripheral serotonin levels eightfold and reduced fatigue by half. Eight times more serotonin. This figure struck me when I first read it, because it sheds completely new light on the link between thyroid and mood. If you’ve read my article on serotonin, you know that this neurotransmitter is at the crossroads of pain, sleep, mood and appetite. And you also know that thyroid patients often have lowered serotonin levels. Carnitine could be a missing link in this equation.
The probable mechanism is indirect but coherent. When mitochondria produce more ATP thanks to the restoration of the carnitine shuttle, overall cellular metabolism improves. The conversion of tryptophan to 5-HTP then to serotonin, which requires energy and cofactors, resumes at a normal pace. The virtuous circle begins: more energy, more serotonin, better sleep, better recovery, less fatigue. And this cascade starts with a derived amino acid that no one ever measures.
According to a study published on Levothyrox-treated patients, twenty percent of hypothyroid patients continue to suffer from fatigue despite appropriate hormonal treatment and normalized blood work. Twenty percent is one patient in five. If TSH is correct, if T4 and T3 are within normal limits, why does this fatigue persist? Carnitine depletion is one of the answers. And it’s perfectly consistent with the limiting factor law that I apply in consultation: even if all thyroid cofactors are corrected, if the mitochondrial shuttle is broken, cells remain in an energy deficit.
The Hyperthyroidism Paradox
This is where carnitine becomes fascinating. If it’s lacking in hypothyroidism and needs to be restored, one might expect it to be contraindicated in hyperthyroidism. It’s the opposite. L-carnitine is one of the rare nutrients that acts as a bidirectional thyroid modulator: it supports cellular function when the thyroid is low, and it slows hormonal action when the thyroid is overactive.

The mechanism is clear. In hyperthyroidism, excess T3 and T4 enters cell nuclei and binds to thyroid nuclear receptors, activating the transcription of genes that accelerate metabolism. This is what causes the tachycardia, weight loss, tremors, excessive thermogenesis, the symptoms I detailed in the article on Graves’ disease. L-carnitine, administered at doses of two to four grams per day, inhibits the entry of T3 and T4 into cell nuclei. It acts like a doorkeeper who filters access: the hormones are still in the blood, but they can no longer exert their nuclear action excessively.
A randomized double-blind placebo-controlled study demonstrated that in hyperthyroid patients, L-carnitine supplementation at two and four grams per day reversed hyperthyroid symptoms and normalized osteocalcin, a marker of bone metabolism that becomes overactive in hyperthyroidism (excess T3 stimulates osteoclasts and weakens bones). This result is remarkable because it shows that carnitine doesn’t alter blood thyroid hormone levels; it modifies their action at the cellular level. This is a crucial distinction. You can have identical blood work before and after taking carnitine, but your cells receive a very different hormonal signal.
For patients with Graves’ disease or non-autoimmune hyperthyroidism, this opens an interesting perspective to complement endocrinological treatment. Carnitine doesn’t replace Neomercazole or conventional monitoring, but it offers a cellular protection mechanism that conventional pharmacology doesn’t provide. And in the thyroid storm that is a hyperthyroid crisis, every metabolic brake counts.
Thyroid Myopathy: When Muscles Waste Away
There is a clinical picture that perfectly illustrates carnitine’s role in thyroid physiology: thyroid myopathy. This term refers to muscle damage that accompanies thyroid dysfunction, and here’s the crucial point: it affects both hypothyroidism and hyperthyroidism. In both cases, muscle carnitine stores are depleted.
In hypothyroidism, myopathy manifests as cramps, diffuse muscle pain, weakness on exertion, abnormally slow recovery after exercise. Patients often describe a sensation of “leaden legs,” an inability to climb stairs without becoming breathless, fatigue that sets in after the slightest physical effort. This is not laziness. It’s a power failure at the cellular level. Myocytes (muscle cells) no longer receive enough fatty acids in their mitochondria, ATP production drops, and the muscle can no longer function normally. It’s the same mechanism I described in the article on fibromyalgia, where Bengtsson measured a twenty percent ATP deficit in the muscles of patients.
In hyperthyroidism, myopathy takes a different but equally debilitating form: muscle wasting (amyotrophy), weakness of proximal muscles (difficulty rising from a chair, lifting arms above the head), sometimes intermittent paralysis. Excess T3 accelerates protein catabolism and carnitine consumption explodes in an attempt to keep up with a runaway metabolism.
In both cases, restoring carnitine stores through supplementation improves the muscle picture. This is not a treatment for the thyroid cause. It’s a support for the terrain at the cellular level that allows the muscle to function while waiting for the thyroid to be corrected. And often, it’s this support that makes the difference between a patient who can stand and a patient who collapses.
Endogenous Synthesis: A Chain of Dependencies
Your body makes approximately twenty-five percent of its carnitine needs. The rest must come from diet. But this endogenous synthesis is itself fragile, because it depends on a cascade of cofactors each of which can become the limiting factor.
Carnitine is synthesized in the liver and kidneys from lysine and methionine, two essential amino acids that your body cannot make. Lysine is found mainly in meat, fish, eggs and legumes. Methionine is present in eggs, fish, Brazil nuts and sesame seeds. A diet poor in animal protein can therefore limit precursors.
But precursors aren’t enough. The transformation of lysine into carnitine requires two hydroxylase enzymes that require vitamin C as an obligatory cofactor. Without vitamin C, no carnitine synthesis. This biochemical link explains one of the most anciently described symptoms in medical history: the extreme fatigue of scurvy. When eighteenth-century sailors died of exhaustion after months at sea without fresh fruit or vegetables, it wasn’t just a collagen problem (the most visible symptom of scurvy). It was also a collapse in carnitine production, and thus a gradual shutdown of fatty acid combustion in mitochondria. The body lost its capacity to produce energy.
Iron also plays a role in the synthesis chain. Low ferritin, a situation I find in the vast majority of thyroid women I see in consultation, can compromise carnitine production. It’s another layer in the thyroid vicious circle: hypothyroidism reduces iron absorption (by lowering gastric acidity), iron deficiency reduces carnitine synthesis, lack of carnitine reduces energy production, and fatigue worsens. Each link weakens the next. Vitamins B6 and B3 round out the list of cofactors. The thyroid micronutrition that I detail in my dedicated article makes full sense here: correcting iron, vitamin C and B vitamins doesn’t just serve the thyroid directly, it also restores the body’s ability to make its own carnitine.
Brain Fog: The Mitochondrial Lead
Brain fog is one of the most frustrating symptoms of hypothyroidism. That sensation of thinking through cotton, searching for words, forgetting why you entered a room, rereading the same sentence three times without understanding it. Patients often describe this symptom with more distress than physical fatigue, because it touches their identity, their capacity for thought, what defines them as individuals.
The brain is an extraordinarily energy-hungry organ. It represents two percent of your body weight but consumes twenty percent of your total energy. Its neurons run mainly on glucose, but they also use ketone bodies as alternative fuel, especially during fasting or carbohydrate restriction. And for neurons to use fatty acids and produce ketone bodies efficiently, they need carnitine.
Acetyl-L-carnitine, the acetylated form of carnitine, is particularly interesting for the brain because it crosses the blood-brain barrier. Once in brain tissue, it serves as a precursor to acetylcholine, the neurotransmitter of memory, learning and concentration. Acetylcholine deficiency is one of the central mechanisms of Alzheimer’s disease, and research on acetyl-L-carnitine in cognitive aging shows encouraging results on working memory and information processing speed.
In hypothyroidism, brain fog results from a convergence of factors: less T3 to stimulate neuronal metabolism, less serotonin to regulate mood and cognition, less carnitine to power brain mitochondria. It’s a triple energy deficit. And correcting the thyroid without restoring carnitine is like repairing two of the three legs of a stool: it still won’t stand.
The Link to the Adrenals
There’s an aspect of carnitine that I rarely see mentioned in micronutrition texts, yet it strongly resonates with my clinical practice. Chronic stress and adrenal exhaustion worsen carnitine depletion through at least three mechanisms.
The first is pregnenolone theft. Pregnenolone, that mother molecule of all steroid hormones, is made from cholesterol in the mitochondria. When the adrenals are overworked by stress, they consume more mitochondrial raw materials, which diverts energy resources at the expense of fatty acid beta-oxidation. Carnitine demand increases while the body is already in economy mode.
The second mechanism goes through cortisol. Chronically elevated cortisol increases hepatic gluconeogenesis (glucose production from proteins and glycerol), which means the liver is diverted from its synthesis functions, including carnitine synthesis. The same liver that should be converting your T4 to T3 and making your carnitine is monopolized by stress management.
The third mechanism is indirect but devastating: chronic stress depletes vitamin C reserves. The adrenals are the organ with the highest concentration of vitamin C in the entire body, and every surge of cortisol and adrenaline consumes vitamin C. A chronically stressed patient burns through their vitamin C, which reduces carnitine synthesis, which reduces energy production, which worsens stress vulnerability. Yet another vicious circle in the complex network linking the adrenals to the thyroid.
What I Propose in Consultation
When I see a thyroid patient whose fatigue persists despite well-conducted hormonal treatment and normalized blood work, carnitine is part of my investigation. Total plasma carnitine measurement is a simple test, covered by insurance, that any laboratory can perform. A value below 25 micromoles per liter in adults strongly suggests depletion.
For supplementation, I distinguish between two situations. In hypothyroidism with persistent fatigue, L-carnitine or acetyl-L-carnitine at one to three grams daily, divided into two doses (morning and noon, never evening as it can be stimulating), is the basic protocol. Acetyl-L-carnitine is my preference when brain fog is foremost, because it crosses the blood-brain barrier and supports acetylcholine production. Base L-carnitine is sufficient when fatigue is essentially muscular.
In hyperthyroidism, the dose is higher: two to four grams daily of L-carnitine, under medical supervision, complementing endocrinological treatment. It’s not a substitute for Neomercazole or antithyroid drugs. It’s a complementary metabolic brake that protects cells from excess thyroid hormones while waiting for treatment to take effect.
In both cases, I systematically correct the cofactors of endogenous synthesis: vitamin C (500 milligrams to one gram daily, away from iron-rich meals), iron if ferritin is low (target 50 to 80 nanograms per milliliter), vitamins B6 and B3, and sufficient protein intake to provide lysine and methionine. It’s the same logic as for the seven thyroid nutrients: without cofactors, the machine won’t run.
I also check the digestive terrain. Leaky gut absorbs carnitine and cofactors poorly. Correcting gut terrain is always a priority, even before talking about supplementation. Giving carnitine to a leaky gut is like filling a bucket with holes.
“All illness is a maturity and not an accident; illness is prepared over a long time by health care faults.” Dr Pache
Food Sources
Red meat remains by far the richest food source of carnitine, with about one hundred milligrams per one hundred grams of beef. The word “carnitine” comes from the Latin carnis, meaning flesh. Lamb provides comparable amounts; pork and chicken about two to three times less. Fish, dairy products and eggs contain modest amounts. Plant foods are extremely poor in carnitine, which explains why strict vegetarian and vegan diets are a risk factor for depletion.
I’m not saying you need to eat red meat every day. I’m saying you need to know this fact and account for it in nutritional counseling. A thyroid patient who doesn’t eat red meat must compensate, either through sufficient intake of lysine and methionine (eggs, fish, legumes paired with whole grains for amino acid complementarity), or through cofactors for endogenous synthesis, or through direct L-carnitine supplementation. This was the case with Isabelle, the patient from the beginning of this article. Four years of strict vegetarian diet without supplementation, with a thyroid running slow. Her plasma carnitine was crashed. Three months of acetyl-L-carnitine at two grams daily, combined with iron and vitamin C correction, transformed her fatigue.
What You Need to Remember
Carnitine is the transporter your mitochondria are waiting for to transform fats into energy. In hypothyroidism, it’s depleted by metabolic slowdown, which worsens fatigue, brain fog and the inability to lose weight. In hyperthyroidism, it slows the action of thyroid hormones at cell nuclei, protecting tissues from excessive stimulation. In both cases, restoring it is part of comprehensive naturopathic support of thyroid terrain.
Its synthesis depends on vitamin C, iron, B6 and B3. All these cofactors are frequently deficient in thyroid patients. Correcting it doesn’t replace hormonal treatment, but it fills a blind spot that Levothyrox alone cannot solve. If your thyroid is treated, if your blood work is good, and you remain fatigued, ask for a plasma carnitine test. The answer could be in this missing link.
To go further, consult my articles on the seven essential thyroid nutrients, on stress and the adrenals and on hypothyroidism as symptom not diagnosis. If you suffer from autoimmune hyperthyroidism, the article on Graves’ disease details the xenoimmune mechanism and the naturopathic protocol.
Want to assess your status? Take the free Claeys thyroid questionnaire in 2 minutes.
If you’d like personalized guidance, you can book a consultation.
To Go Further
- Vitamin B2 (Riboflavin): Your Mitochondria Won’t Run Without It
- Iron: The Silent Deficiency That Exhausts Your Body
- Low Ferritin and Hair Loss: The Link Your Doctor Ignores
- Hypothyroidism Is a Symptom, Not a Diagnosis
Sources
- Benvenga, S. et al. “Usefulness of L-Carnitine, a Naturally Occurring Peripheral Antagonist of Thyroid Hormone Action, in Iatrogenic Hyperthyroidism.” Journal of Clinical Endocrinology and Metabolism 86, no. 8 (2001): 3579-3594.
- Benvenga, S. et al. “Effects of L-Carnitine on Thyroid Economy.” Annals of the New York Academy of Sciences 1033 (2004): 158-167.
If you need personalized support, you can book a consultation. I consult in my Paris office and via video throughout France.
Based in Paris, I consult via video throughout France. For quality thyroid supplementation (L-carnitine, acetyl-L-carnitine, vitamin C, B complex), Sunday Natural (10% off with code FRANCOIS10). The juice extractor supports liver drainage essential to carnitine synthesis and T4-T3 conversion.





Laisser un commentaire
Sois le premier à commenter cet article.