Graves’ Disease: Understanding the Overstimulated Thyroid
Nathalie is thirty-six years old. She came to consult with me because her heart was beating too fast. Not after exercise, not after a fleeting moment of stress. At rest, lying in her bed in the evening, ninety-six beats per minute. Her doctor had first thought of anxiety. She was prescribed Lexomil. Then a cardiologist checked her heart, normal ECG, normal Holter monitor, reassuring conclusion. But the tachycardia persisted. She had lost five kilos in two months without changing her diet. Her hands trembled when she held a cup of coffee. She sweated at night. And one morning, looking at herself in the mirror, she noticed that her eyes seemed larger than usual, as if her gaze had opened wider.
It was an endocrinologist, consulted six months after the first symptoms, who finally made the diagnosis: Graves’ disease. TSH collapsed at 0.01 mU/L, free T4 at three times normal, antibodies against TSH receptor (TRAb) positive. She was prescribed Neomercazole and told that if the treatment didn’t work within eighteen months, she would need to consider radioactive iodine or surgery. No one mentioned her intestines. No one asked if she had experienced major stress in the months preceding the onset of symptoms. And no one explained why her own immune system had begun frantically stimulating her thyroid instead of destroying it.
If you’ve read my article on Hashimoto, you already know the other face of thyroid autoimmunity: the one that destroys. Graves’ is the exact mirror image. Where Hashimoto produces destructive antibodies that demolish the thyroid cell by cell, Graves’ produces stimulating antibodies that force it to run at full capacity, day and night, without brakes. And it is precisely this difference that makes Graves’ both louder and more dangerous in the short term.
What Graves’ Disease Does to Your Body
Graves’ disease affects approximately one percent of the French population, or nearly seven hundred thousand people. The ratio is four women to one man, and it strikes preferentially young adults between twenty and forty years old. Concordance studies in monozygotic twins show a rate of only twenty-two percent[^1], which means that genetics alone is insufficient: an environmental trigger is needed for the disease to manifest. The HLA-DR3 gene is most frequently associated with Graves’, but its presence is neither necessary nor sufficient.

To understand what happens in the body of someone with Graves’ disease, you must first understand the thyroid thermostat. Normally, the pituitary gland secretes TSH which binds to a specific receptor on the surface of thyroid cells. This receptor, when activated by TSH, orders the thyroid to manufacture T4 and T3 hormones. When the hormone level is sufficient, the pituitary reduces TSH, and the thyroid slows down. This is an elegant and precise feedback loop.
In Graves’ disease, this loop is short-circuited. TRAb antibodies bind to the TSH receptor exactly as TSH itself would, but with one crucial difference: they are not subject to any feedback control. The pituitary may cut TSH (hence the collapsed TSH in lab results), but the TRAb antibodies continue to stimulate the thyroid permanently. It’s as if someone stuck the accelerator of your car and disconnected the brake. The engine races.
The consequences are systemic. The heart accelerates because thyroid hormones directly increase heart rate and myocardial contractility. Resting tachycardia, often above ninety beats per minute, is the most frequent and earliest sign. In five to ten percent of patients, this acceleration degenerates into atrial fibrillation, a potentially serious arrhythmia that by itself justifies cardiac monitoring. Basal metabolism increases by thirty to sixty percent, which explains rapid weight loss despite normal or increased appetite. Thermogenesis runs wild: sweating, heat intolerance, clammy hands. Transit accelerates with frequent stools or diarrhea. Muscles waste away (thyroid myopathy). Bones weaken because excess T3 stimulates osteoclasts. And the nervous system runs in overdrive: nervousness, irritability, insomnia, fine tremors of the extremities.
What your doctor calls hypothyroidism is often a tired, slowed thyroid. Graves’ disease is the exact opposite: a runaway thyroid, driven by antibodies that obey no one.
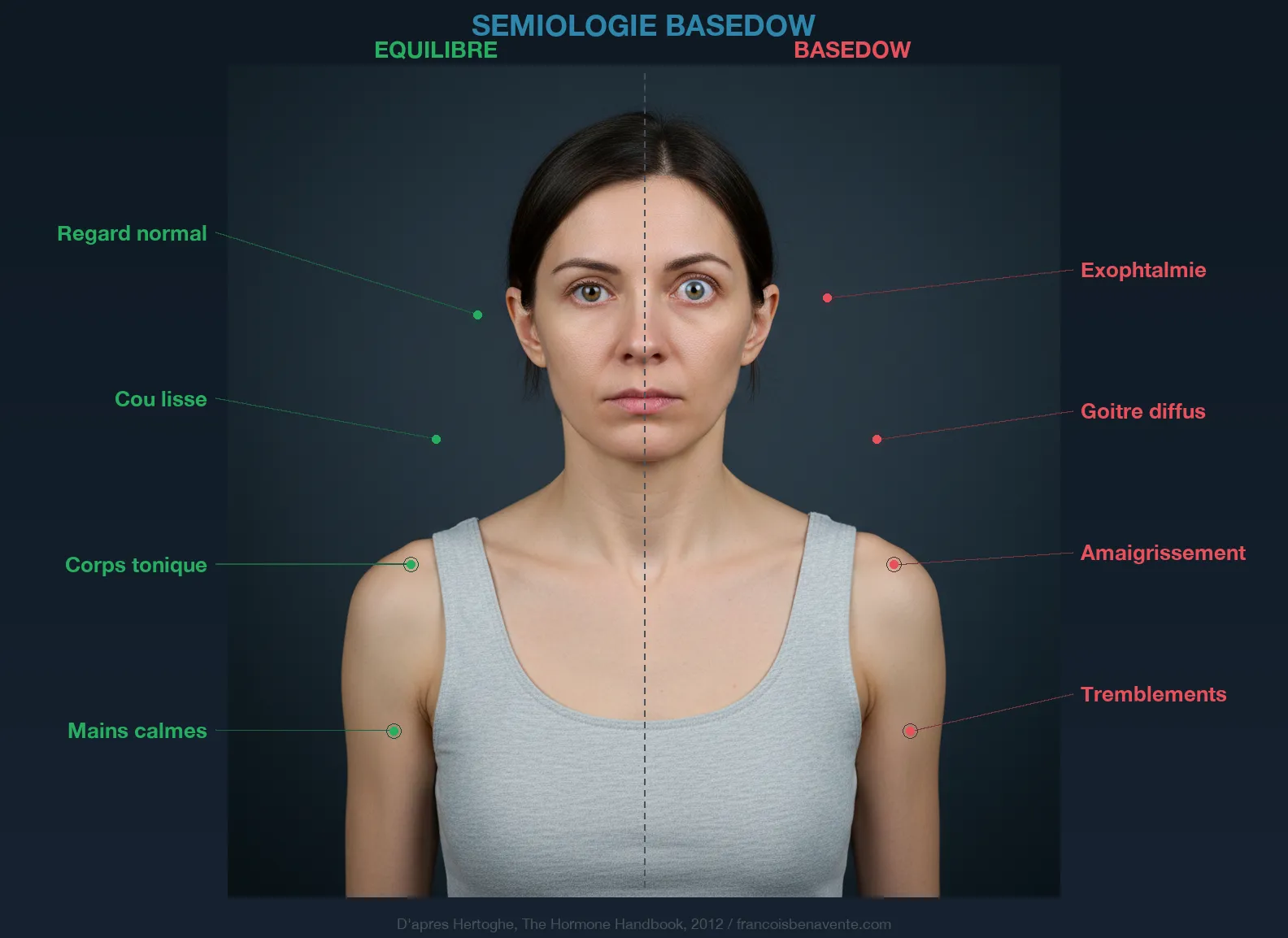
Exophthalmos: When the Eyes Tell the Story
Exophthalmos in Graves’ disease (eyes that seem to protrude from their sockets) is perhaps the most characteristic and most feared sign of the disease. It affects approximately fifty percent of patients and can appear before, during, or even after treatment of hyperthyroidism. Its mechanism is fascinating and reveals how far autoimmunity can strike from its target organ.
Behind the eyeball lies retro-orbital adipose tissue that is normally discreet. In Graves’ disease, this tissue becomes the scene of a true immune invasion. CD4+ T cells, CD8+ T cells, B lymphocytes and macrophages infiltrate the retro-orbital fat. Local fibroblasts become activated and begin to produce massive amounts of glycosaminoglycans, molecules that attract water like a sponge. In parallel, fibroblasts differentiate into adipocytes, increasing the volume of orbital fat. The result is progressive swelling of the retro-orbital tissue that pushes the eyeball forward.
This ocular involvement can range from simple aesthetic discomfort (a slightly more open gaze, an impression of fixity) to severe complications: dry eyes from incomplete eyelid closure, diplopia from involvement of the eye muscles, and in extreme cases, compression of the optic nerve with risk to vision. It is one of the strongest arguments for not neglecting Graves’ disease and for acting on the immune terrain as early as possible.
The Xenoimmune Mechanism: Yersinia and Molecular Mimicry

Professor Seignalet proposed for Graves’ disease a xenoimmune mechanism that differs subtly from the one he describes for Hashimoto, and this difference is crucial. In Hashimoto, foreign peptides accumulate in thyrocytes and trigger a destructive immune response. In Graves’ disease, the mechanism is based on molecular mimicry with a specific intestinal bacterium: Yersinia enterocolitica.
Yersinia enterocolitica is a gram-negative bacterium that colonizes the intestine and carries on its surface a lipoprotein whose epitope (an amino acid sequence) is structurally homologous to the TSH receptor on thyroid cells. When the immune system manufactures antibodies against this Yersinia lipoprotein (which is perfectly normal, it’s its job), these antibodies will cross-react with the TSH receptor. And instead of destroying, they stimulate. This is the whole particularity of Graves’ disease: the antibody behaves like an agonist, not an antagonist. It mimics TSH.
Seignalet makes an important point: the bacterium itself does not need to cross the intestinal barrier. A simple peptide suffices. A fragment of this lipoprotein that passes through a leaky intestine can be captured by antigen-presenting cells and trigger the entire immune cascade. This is why intestinal permeability remains the starting point, as in all autoimmune diseases Seignalet studied. And this is why the hypotoxic diet and intestinal repair are as relevant in Graves’ disease as in Hashimoto, even though the antibody produced is of very different nature.
This theory also explains why conventional treatments, as effective as they are at controlling hyperthyroidism in the short term, do not cure Graves’ disease. Synthetic antithyroid drugs (Neomercazole, Thyrozol) slow hormone production, but do not touch the underlying immune mechanism. Result: more than fifty percent of relapses within three years of stopping treatment. Radioactive iodine and surgery destroy the thyroid, which resolves hyperthyroidism but creates permanent hypothyroidism requiring Levothyrox for life. None of these approaches tackle the intestine, dysbiosis, stress, or molecular mimicry.
The Hashimoto-Graves’ Switch
There is a phenomenon that endocrinologists know well but explain poorly: the switch from one form of thyroid autoimmunity to the other. A Hashimoto patient on Levothyrox who suddenly develops palpitations, weight loss, and excessive nervousness. Or conversely, a treated Graves’ patient who evolves toward autoimmune hypothyroidism with anti-TPO antibodies that climb. This switch is documented in the literature and has nothing mysterious about it when you understand Seignalet’s mechanism.
The thyroid is a target organ. Antibodies are the weapons. And the leaky intestine is the factory that manufactures ammunition. Depending on the type of peptide that crosses the intestinal barrier, depending on the patient’s HLA genetic predisposition, depending on the nature of dysbiosis (with or without Yersinia), the immune system will produce destructive antibodies (Hashimoto) or stimulating antibodies (Graves’). Sometimes both coexist, and the balance between them determines the clinical picture at any given moment. If you want to understand how feminine hormones influence this switch, excess estrogen modifies the Th1/Th2 balance and can promote the transition from one profile to another.
This phenomenon has a major clinical implication: monitoring TSH alone is insufficient. A complete workup should include anti-TPO, anti-thyroglobulin, and anti-TSH receptor antibodies (TRAb) to map the entire autoimmune profile. The seven thyroid nutrients that I detail in my dedicated article remain the fundamental cofactors in both cases, but the therapeutic approach differs: you stimulate a tired thyroid, you calm a runaway thyroid.
Stress, the Major Trigger
Studies by Rosch published in 1993 are conclusive: stress is found as a triggering factor in more than ninety percent of Graves’ disease cases. This figure is staggering. It means that in virtually all cases, a major stressful event preceded the onset of the disease: a death, a divorce, job loss, an accident, a move, intense family conflict.
Nathalie, my patient from the beginning of this article, confirmed this pattern to me. Six months before her first symptoms, she had experienced separation from her partner after eight years of living together, coupled with a legal conflict over custody of her son. When I asked her the question, she shrugged: “Yes, but what does that have to do with my thyroid?” The connection is direct.
Chronic stress acts on the thyroid through at least four interconnected mechanisms. The first is dysregulation of the hypothalamic-pituitary-adrenal axis. Chronically elevated and then collapsed cortisol modifies the Th1/Th2 immune balance, promoting Th2 autoimmune responses which are precisely those involved in antibody production such as TRAb. The second is increased intestinal permeability. Cortisol and adrenaline divert blood flow from the intestine to muscles (fight or flight response), which starves the intestinal mucosa and loosens tight junctions. The third is pregnenolone theft: under intense stress, all available pregnenolone is channeled toward cortisol manufacture at the expense of progesterone and DHEA, which alters the hormonal and immune environment. The fourth is modification of the microbiota. Chronic stress alters the composition of intestinal flora, favoring pathogenic species at the expense of protective bacteria.
This is why Dr. Jean Du Chazaud, founder of endopsychology, wrote that “the thyroid is the gland of emotion.” This sentence takes on particular meaning in the context of Graves’ disease. The thyroid does not fall ill by chance. It falls ill when unprocessed emotions overwhelm the terrain.
The Naturopathic Protocol: Calming the Storm

The protocol I propose in consultation for Graves’ disease differs from that for Hashimoto on one fundamental point: here, you do not stimulate the thyroid, you calm it. But the foundation remains the same: repair the intestine, modulate immunity, support the terrain. I organize this approach into six axes inspired by my global thyroid strategy: relax, reanimate, recharge, eliminate, nourish, measure.
The first axis is the hypotoxic diet. Seignalet recommends starting with a proportion of twenty percent detoxifying and eighty percent revitalizing, then progressively evolving toward fifty-fifty. In practice, this means eliminating gluten and dairy products (same pattern as for Hashimoto, since the leaky intestine is the common denominator), cooking below 110 degrees, prioritizing organic foods and raw virgin oils. The specificity for Graves’ disease is to model the diet on dysbiosis: if stool analysis or food IgG testing reveals specific intolerances, these should be integrated into the protocol. Individualization through IgG testing of foods, as Wentz recommends (forty percent success versus twenty-five percent for Seignalet diet alone), multiplies the effectiveness of the approach.
The second axis is thyroid-slowing phytotherapy. This is where Graves’ disease is radically distinguished from Hashimoto. Three plants possess documented thyroid-slowing action. Lycopus (Lycopus europaeus) inhibits TSH binding (and therefore TRAb) to its receptor and reduces peripheral conversion of T4 to T3. Melissa (Melissa officinalis) blocks TSH fixation on thyrocytes and exerts precious anxiolytic effect in this context of nervousness. Gromwell (Lithospermum officinale) contains lithospermic acid which directly inhibits thyroid hormone synthesis. In combined infusion, two to three cups per day, these three plants constitute a soft and physiological brake that complements the action of synthetic antithyroid drugs without replacing them. This is never about stopping medical treatment in favor of plants, but supporting the terrain while medicine controls the emergency.
The third axis is adrenal support. Exhausted adrenals do not allow the thyroid to regain its balance, whether in hypo or hyperthyroidism. Essential oil of Scots pine or mountain savory applied to the adrenal area (at the lumbar level, at the level of the kidneys) twice a day stimulates the adrenal cortex. Adaptogenic plants (rhodiola, ashwagandha, eleuthero) help the body regain its capacity to adapt to stress, but ashwagandha must be handled with caution in Graves’ disease because it contains withanolides that can stimulate the thyroid. In this case, rhodiola and eleuthero are preferable. Magnesium bisglycinate at 300 to 400 milligrams per day is essential: chronic stress depletes magnesium reserves, and magnesium is indispensable for the functioning of more than three hundred enzymes, including those involved in cortisol regulation.
The fourth axis is detoxification. Substances harmful to the thyroid are well identified: heavy metals (mercury from dental amalgams, lead, cadmium), fluoride present in tap water and toothpastes, endocrine disruptors in daily life. Liver detoxification is all the more important because the liver is the primary site of T4 to T3 conversion, and an overburdened liver cannot properly metabolize excess circulating thyroid hormones. Fresh vegetable juices from a cold-press juicer (carrot, beet, celery, ginger) support both phases of liver detoxification. You must also eliminate inhibitors of T4/T3 conversion: tea, coffee, gluten, cigarettes, alcohol. “Primum non nocere,” as Hippocrates said. Stopping intoxicating the body is the first form of healing.
The fifth axis is the emotional and artistic dimension. This is an axis that conventional medicine completely ignores, but naturopaths know well. Chazaud wrote that the thyroid vibrates with emotions, that it races when unexpressed emotions accumulate, and that it calms when given an outlet for them. Artistic activity (painting, music, singing, dancing, writing) is not a soul supplement in the protocol: it is a therapeutic tool. When I tell a Graves’ patient to sign up for a pottery class or take up the guitar again, it is not to fill her schedule. It is because positive emotional stimulation acts directly on the neuroendocrine axis and modulates the immune response. Carton said: “Each digestion is a battle.” One could add: each repressed emotion is a battle the thyroid fights in your place.
The sixth axis is hydrotherapy. The alternation of hot and cold (Scottish shower, sauna followed by cold shower, daily cold arm bath) stimulates the adrenals, relaunches lymphatic circulation and strengthens the adaptive response of the body according to the principles of Kneipp and Salmanoff. Gentle thyroid massage with myrrh essential oil, in downward movement (and not upward as in hypothyroidism), twice a day, is an empirical technique used by several naturopaths to calm glandular activity.
Cofactors to Monitor
Supplementation in Graves’ disease requires more caution than in Hashimoto. Some cofactors that stimulate the thyroid (iodine, certain forms of tyrosine) are contraindicated in active hyperthyroidism. Others remain essential.
Selenium is the first cofactor to restore. At 100 to 200 micrograms per day of selenomethionine, it protects the thyroid against the intense oxidative stress generated by hormone overproduction, participates in selenoprotein function and helps modulate the autoimmune response. Zinc as bisglycinate, 15 to 30 milligrams per day, is essential for the vitamin D receptor (VDR gene) and immune regulation. Vitamin D at 2000 to 4000 IU per day depending on labs is a first-line immunomodulator whose deficiency aggravates all autoimmune processes. Omega-3 EPA/DHA in fish oil or capsules (2 to 3 grams per day) calm systemic inflammation. Magnesium, already mentioned for the adrenals, is doubly important because hyperthyroidism accelerates its renal elimination.
One often overlooked point: testosterone, in men as in women, participates in regulating T3 and T4 production. A deficit in testosterone can perpetuate thyroid imbalance. In women, the link between estrogen, progesterone and thyroid is particularly intertwined: excess estrogen (estrogenic dominance) increases TBG (thyroid hormone transport protein) and modifies the immune profile.
For quality thyroid supplementation, Sunday Natural offers selenium, zinc and vitamin D in highly bioavailable forms, with ten percent off using code FRANCOIS10.
Thyroid Morphotype and the DIO2 Gene
Daniel Kieffer distinguishes two major morphotypes in naturopathy: the retracted and the dilated. In Graves’ disease, the retracted profile (slender, nervous, catabolic) is more frequent than in Hashimoto. This patient consumes more than he stores, burns his reserves, fidgets, loses weight. His sympathetic nervous system dominates. Naturopathic strategy must take this into account: no additional stimulation, but calm, parasympathetic tone, yin. Relaxation techniques (heart rate variability, meditation, gentle yoga), a diet rich in tryptophan to support serotonin (banana, turkey, brown rice, cashews), and a rhythm of life that respects biological clocks.
The DIO2 gene deserves to be tested in the context of Graves’ disease as well. This gene codes for type 2 deiodinase, the enzyme that converts T4 to active T3. If the patient carries the Thr92Ala variant, his T4/T3 conversion is impaired, which can paradoxically mask the severity of hyperthyroidism at the peripheral level while maintaining a very elevated T4 in the blood. Mouton recommends this test to adjust therapeutic strategy. Since the liver is the primary site of conversion, a complete liver workup (transaminases, GGT, cholesterol) is part of the baseline assessment. Hyperthyroidism classically lowers total cholesterol, which can falsely reassure the doctor when it is actually a sign of thyroid overfunctioning.
What to Avoid
Certain mistakes are common and can worsen Graves’ disease.
The first is to supplement with iodine. In simple hypothyroidism, iodine can be beneficial under supervision. In Graves’ disease, iodine is fuel that feeds the fire. The more iodine the thyroid has available, the more hormones it produces under stimulation by TRAb. Excess iodine also increases intrathyroidal oxidative stress via the Fenton reaction. Be careful with iodine-rich seaweeds (kombu, wakamé, nori), multivitamin supplements containing iodine, and iodine-contrast agents used in medical imaging.
The second mistake is to stimulate the thyroid with plants or thyroid-stimulating nutrients. Ashwagandha (Withania somnifera), so precious in hypothyroidism, is potentially problematic in Graves’ disease. Guggul, forskolin, and preparations containing tyrosine should be avoided in the active phase.
The third mistake is to neglect medical follow-up. Graves’ disease is not a condition to manage alone with herbal tea. Tachycardia can degenerate into atrial fibrillation. Exophthalmos can threaten vision. Thyrotoxicosis (acute hyperthyroidism crisis) is a vital emergency. Synthetic antithyroid treatment is often necessary at first to control the hormonal storm. Naturopathy intervenes as a complement, to treat the terrain and reduce the risk of relapse which remains, without intervention on the root causes, greater than fifty percent within three years.
The fourth mistake is to ignore sleep. Hyperthyroidism generates sleep-onset insomnia (the body is too stimulated to shut down) which worsens stress, which worsens autoimmunity, which worsens hyperthyroidism. Breaking this cycle involves strict sleep hygiene: total darkness, cool room, no screens after nine p.m., and if necessary sedating plants (valerian, passionflower, California poppy) or low-dose melatonin (0.5 to 1 milligram) to help regain physiological sleep onset.
The Workup Your Doctor Should Prescribe
If you suspect Graves’ disease or already have a diagnosis, a complete blood workup is essential. TSH alone is insufficient, as in all thyroid pathologies. You must measure free T3 and free T4 to quantify hyperthyroidism, all three antibodies (anti-TPO, anti-thyroglobulin and especially TRAb which is the specific marker for Graves’), ultrasensitive CRP to assess low-grade inflammation, vitamin D, selenium, zinc, red blood cell magnesium, ferritin, active B12, and homocysteine.
Salivary cortisol testing at four points in the day (morning upon waking, noon, four p.m., ten p.m.) is essential to assess adrenal status. Complete liver workup and lipid profile allow you to check liver function and detect the hypocholesterolemia characteristic of hyperthyroidism. And IgG testing of major foods helps individualize the avoidance diet beyond simple gluten and dairy elimination.
Returning the Body the Capacity to Regulate Itself
Professor Seignalet, in his clinical results on thyroid autoimmune diseases, was always of disarming honesty. He never claimed to cure. He showed that the hypotoxic diet could extinguish the autoimmune process and allow the body to regain a certain balance. In Graves’ disease, this approach has a considerable advantage over Hashimoto: the thyroid is not destroyed, it is overstimulated. If you stop stimulating it (by calming autoimmunity, repairing the intestine, reducing stress, eliminating cross-reactive antigens), it can return to normal functioning. This is a fundamental difference. In Hashimoto, destroyed cells do not come back to life. In Graves’ disease, the cells are intact, they are just overvoltaged.
This does not mean Graves’ disease is easier to treat. The acute phase is more dangerous than Hashimoto (the heart, the eyes, metabolism), and medical follow-up is absolutely essential. But it means that the potential for recovery is better if you act on the terrain in parallel with conventional treatment.
I think of Nathalie, who came back to see me six months after our first consultation. Her Neomercazole had stabilized her thyroid. But it was the combination of the gluten and dairy-free diet, infusions of lycopus and melissa, resuming piano (which she had abandoned ten years earlier), morning and evening heart rate variability, and supplementation with selenium, zinc and magnesium that had lowered her TRAb by sixty percent. Her endocrinologist was amazed. Not me. When you give the body the conditions to regulate itself, it regulates itself.
Want to assess your status? Take the free Claeys thyroid questionnaire in 2 minutes.
If you want personalized support, you can book a consultation.
To Learn More
- Graves’ Disease: Preventing Relapse After Neomercazole
- Graves’ and Eyes: Protecting Your Vision Naturally
- Hashimoto: The Overlooked Causes Your Doctor Isn’t Looking For
- Iodine and Autoimmune Thyroid: Danger or Benefit? Truth and Fiction
Sources
- Seignalet, Jean. L’Alimentation ou la Troisième Médecine. 5th ed. Paris: François-Xavier de Guibert, 2004.
- Rosch, Paul J. “Stressful Life Events and Graves’ Disease.” Lancet 342 (1993): 566-567.
- Wentz, Izabella. Hashimoto’s Protocol. New York: HarperOne, 2017.
- Mouton, Georges. Écologie digestive. Marco Pietteur, 2004.
- Carton, Paul. Traité de médecine naturiste. Le François, 1920.
If you want personalized support for Graves’ disease or any other thyroid pathology, you can book a consultation. I consult in office in Paris and by video throughout France. You can also contact me with any questions.
To learn more, my complete thyroid training covers everything I’ve written in my thyroid articles with case studies, commented workups, and detailed protocols. And if you’re looking for the basics of naturopathy to understand the concept of terrain and detoxification pathways, it’s the best starting point.
For thyroid supplementation, Sunday Natural offers pharmaceutical-quality selenium, zinc and vitamin D (ten percent off with code FRANCOIS10). The Inalterra grounding mat reduces nighttime autoimmune inflammation (ten percent off with code FRANCOISB). Find all my partnerships with exclusive promo codes.
Graves’ disease is not a death sentence. It’s an alarm signal. Your body is telling you that something is dysfunctional in your intestine, your immunity, your stress management, your environment. Neomercazole extinguishes the fire. But if you want the fire not to return, you need to find who lit the match. And this search is exactly what naturopathy proposes to do.








Laisser un commentaire
Sois le premier à commenter cet article.