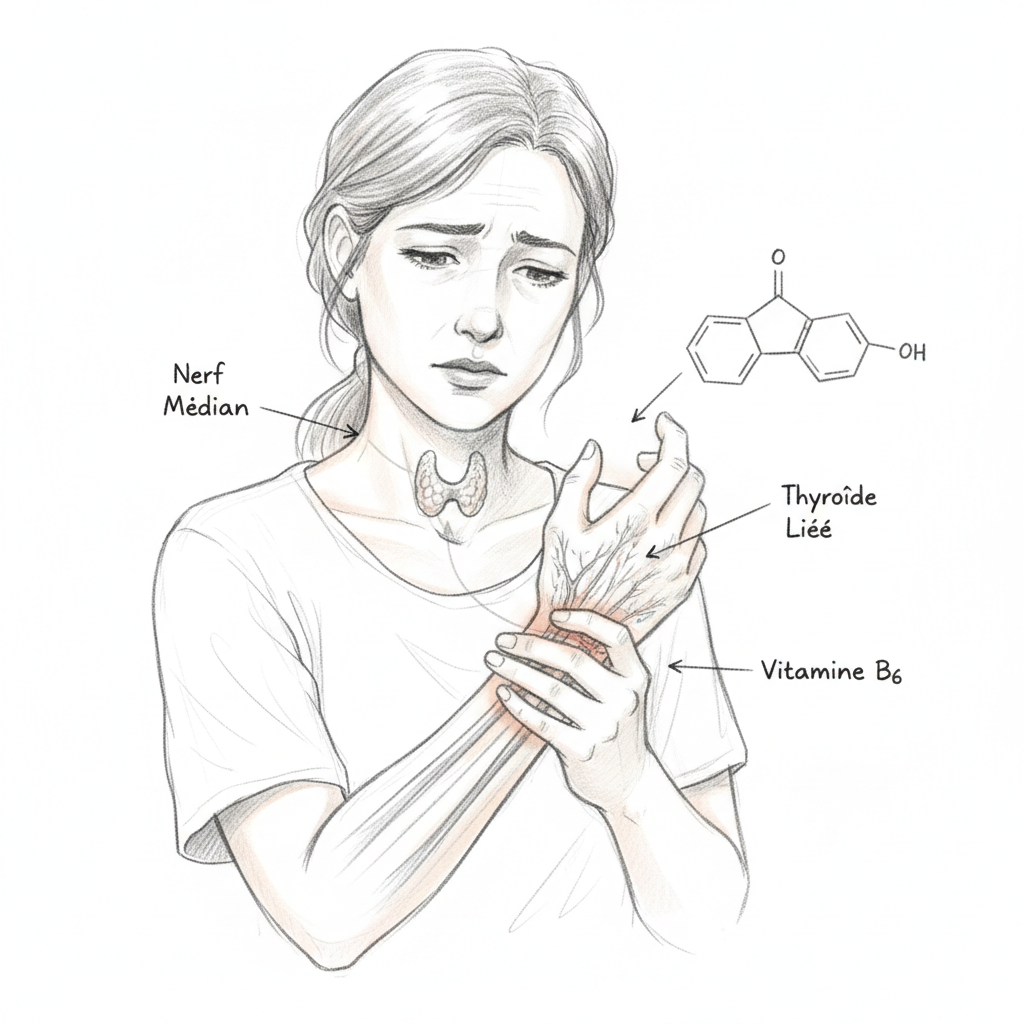
Isabelle is forty-nine years old and wakes up every night with numb hands. The first three fingers of each hand (thumb, index, middle finger) feel dead, insensitive, with tingling that takes ten minutes to fade when she shakes her hands. It started a year ago, first in her right hand, then in both. Her doctor diagnosed bilateral carpal tunnel syndrome and referred her to a surgeon. The electromyogram confirmed moderate compression of the median nerve at both wrists. The surgeon proposed surgery. Isabelle asked for time.

When she came to my consultation, I noticed several things. A puffy face in the morning (which she attributed to cellular aging). Fine hair that was falling out (which she attributed to perimenopause). A weight gain of five kilos in one year (which she attributed to lack of exercise). Constipation that was settling in (which she attributed to stress). And permanent fatigue (which she attributed to everything). None of her doctors had made the connection between these symptoms and her numb hands.
I ordered a complete thyroid panel. TSH at 4.2 mIU/L (“normal” according to the lab, but functionally elevated). Free T4 in the lower third. Low free T3. Anti-TPO at 210. Hashimoto. And collapsed serum vitamin B6 (below normal). Isabelle’s carpal tunnel was not an isolated mechanical problem. It was a symptom of undiagnosed hypothyroidism, worsened by B6 deficiency.
Six months later, on Levothyroxine (prescribed by her doctor after the panel), P5P 50 mg daily, magnesium 400 mg at bedtime and night splint, the numbness had decreased by 80%. The surgeon agreed to delay surgery. A year later, the symptoms had completely disappeared. Isabelle was never operated on.
Myxedema: when the thyroid swells tissues
To understand why hypothyroidism causes carpal tunnel, we must understand myxedema. In hypothyroidism, the synthesis and degradation of mucopolysaccharides (or glycosaminoglycans, GAG) become unbalanced. GAGs accumulate in connective tissues, trapping water through their strong hygroscopic capacity. The result is thickening and swelling of soft tissues throughout the body.
This myxedema affects all connective tissues, but it is particularly problematic in narrow anatomical spaces. The carpal tunnel is a rigid bony tunnel at the wrist level, bordered by carpal bones behind and the annular ligament in front. Through this tunnel of less than one centimeter in diameter pass nine flexor tendons and the median nerve. When tendon sheaths thicken through myxedematous infiltration, the available space for the nerve decreases and compression sets in.
This is why carpal tunnel is found in 30 to 40% of untreated hypothyroid patients. It is one of the most frequent manifestations of hypothyroidism, yet one of the least sought after. Orthopedic surgeons perform thousands of carpal tunnel surgeries each year without ever testing the thyroid.
Hertoghe, in his clinical treatise, classifies carpal tunnel among the “minor physical signs” of hypothyroidism, in the same way as swollen ankles, puffy eyelids in the morning and moon face. “A bilateral carpal tunnel in a woman over forty should be considered hypothyroid until proven otherwise. Thyroid testing should precede electromyography, not the reverse.”
Vitamin B6: the nerve protector
Vitamin B6 is involved in more than 150 enzymatic reactions in the body. For the nervous system, it is essential for the synthesis of myelin sheaths (nerve insulation), the production of neurotransmitters (serotonin, GABA, dopamine) and the management of nerve inflammation (via prostaglandin modulation).
B6 deficiency makes nerves more vulnerable to mechanical compression. The median nerve, already compressed in a carpal tunnel narrowed by myxedema, suffers doubly when its myelin is weakened by B6 deficiency. This is the “double blow” found in many thyroid patients: hypothyroidism swells tissues AND B6 deficiency (frequent in women on contraceptive pills, in perimenopause or in hypothyroidism) weakens the nerve.
Ellis et al. published in the 1980s and 1990s several studies showing that B6 supplementation (100-200 mg/day of pyridoxine) significantly improved carpal tunnel symptoms in 68 to 85% of patients, with an onset of action of six to twelve weeks. These studies were criticized for their methodology (lack of double-blind in some), but the clinical results are consistent and reproducible.
In naturopathy, I prefer to use P5P (pyridoxal-5’-phosphate), the active form of B6, at a dose of 50 to 100 mg per day. P5P does not require liver conversion (unlike pyridoxine which must be activated by the liver, often overloaded in thyroid patients) and does not present the risk of peripheral neuropathy associated with high doses of pyridoxine (above 200 mg/day long-term).
Other metabolic causes of carpal tunnel
Hypothyroidism and B6 deficiency are not the only metabolic causes. Diabetes and insulin resistance cause peripheral neuropathy and water retention that worsen compression. Pregnancy (hormonal water retention, B6 deficiency from increased demand) explains the frequency of carpal tunnel in the third trimester. Estrogen dominance promotes water retention and thickening of connective tissues. Acromegaly (excess growth hormone) is a rare but classic cause. And magnesium deficiency contributes to muscle spasms and nerve irritability that worsen symptoms.
In my practice, every patient presenting with carpal tunnel benefits from testing that includes a complete thyroid panel, fasting blood glucose and insulin, vitamin B6 (or its functional marker, urinary xanthurenic acid), red blood cell magnesium, vitamin D and female hormone panel if a woman in perimenopause.
The naturopathic protocol
The first step is to treat the cause. If hypothyroidism is identified, medical treatment (Levothyroxine or natural thyroid hormone) is the priority. Resolution of myxedema takes four to eight weeks after normalization of thyroid hormones. If insulin resistance is present, low glycemic index diet, myo-inositol and exercise are the first tools.
The second step is correcting deficiencies. P5P 50 to 100 mg daily (active B6, no liver conversion needed). Magnesium citrate 400 mg at bedtime (anti-spasm and nerve anti-inflammatory effect). Zinc 30 mg daily (cofactor for B6 conversion to P5P and myelin synthesis). Vitamin D 4000 IU daily if level is below 40 ng/mL (D modulates nerve inflammation). Omega-3 EPA/DHA 2 g daily (nerve anti-inflammatory).
The third step is local support. Night wrist splint (keeps wrist in neutral position and reduces compression during sleep, when symptoms are most frequent). Carpal tunnel massage (anterior wrist) with arnica and wintergreen oil (topical anti-inflammatories). Green clay poultice on the wrist (20 minutes, three times a week) to drain local edema. Median nerve gliding exercises twice daily to maintain nerve mobility in the tunnel.
The fourth step is managing water retention. Reduction of table salt (but maintaining unrefined salt in reasonable quantity). Increased dietary potassium (banana, avocado, green vegetables). Lymphatic drainage (dry brushing, exercise, deep breathing). Gentle draining herbs (cherry stem, pilosella, orthosiphon) in daily infusion.
When to consult the surgeon
Carpal tunnel surgery (section of the annular ligament) is indicated when the damage is severe and there is a risk of irreversible nerve damage. Signs of severity are atrophy of the thenar eminence (the large muscle at the base of the thumb that wastes away), permanent loss of sensation (not just nocturnal but also daytime), loss of grip strength (objects falling from hands), and EMG showing axonal degeneration (not just slowing of conduction velocity).
In these cases, surgery is legitimate and should not be delayed. The median nerve, compressed too long, can suffer irreversible damage. The naturopathic protocol then becomes a post-operative complement (accelerate nerve healing with B6, omega-3 and zinc) and prevention of recurrence (treat the underlying metabolic cause).
Warning
Carpal tunnel syndrome can mask other neurological conditions (cervical radiculopathy, diabetic neuropathy, multiple sclerosis). Atypical symptoms (pain radiating into the forearm and shoulder, weakness of the entire arm, symptoms in the fourth and fifth fingers) should raise suspicion of differential diagnosis and lead to a complete neurological evaluation.
Vitamin B6 (pyridoxine) at high dose (above 200 mg/day) over a long period can itself cause peripheral neuropathy (paradox). This is why P5P (active form) is preferable: it is effective at lower doses (50-100 mg) and does not present this risk. Do not exceed 100 mg of P5P per day without professional monitoring.
Kousmine, in her practice of nutritional medicine, observed that “most canal syndromes are signs of nutritional deficiency before being mechanical problems. Treating carpal tunnel with surgery without correcting the nutritional terrain is like patching a leak without repairing the plumbing. The leak will return, elsewhere or in the same place.” Isabelle, who kept both her wrists intact, would confirm this.
Want to evaluate your status? Take the free Claeys thyroid questionnaire in 2 minutes.
If you want personalized support, you can book a consultation.
To go further
- Graves disease and heart: calming the cardiac storm
- Graves disease and pregnancy: conceiving and carrying safely
- Graves disease and stress: the thyroid of emotion
- Estrogen dominance: when your hormones trap your thyroid
Want to evaluate your status? Take the free vitamin B6 deficiency questionnaire in 2 minutes.




Laisser un commentaire
Sois le premier à commenter cet article.