Nathalie is forty-seven years old. She came to see me after three years of recurrent urinary tract infections. Four, five, sometimes six episodes per year. Every time the same ritual: urinary burning, trips to the emergency room or to the doctor, urine cultures, antibiotics. Fosfomycin in a single dose, then norfloxacin when fosfomycin was no longer sufficient, then amoxicillin-clavulanic acid when fluoroquinolones were discouraged. Three years of cascading antibiotic therapies, and the urinary tract infections always came back. But it wasn’t for the urinary tract infections that she came to my office. It was because in the meantime, everything else had fallen apart. Chronic fatigue that pinned her to the couch from three o’clock in the afternoon. Permanent, diffuse anxiety, without any identifiable cause. Bloating after every meal, foul-smelling gas, constipation alternating with loose stools. Eczema on her hands that no longer responded to cortisone. In three years, no one had asked her the simplest question: what if it all came from the same place?
Her intestine.

The human microbiome is a number that makes you dizzy: one hundred thousand billion micro-organisms. Ten times more germs than cells in your body. An ecosystem so complex that some researchers consider it an organ in its own right, an organ that medicine has long ignored because it couldn’t be palpated, radiographed, or dissected on an anatomy table.
“The intestine is the engine of disease.” Catherine Kousmine
Kousmine understood this seventy years ago. Seignalet demonstrated it in Food or the Third Medicine. Marchesseau made it the cornerstone of his orthodox naturopathy. And yet, in 2026, the majority of patients I see in consultation have never heard of their intestinal flora except in yogurt commercials.
The invisible ecosystem that governs you
Your intestine is about two meters long. Its mucous membrane, if completely unfolded, would cover a surface area of two hundred square meters. That’s equivalent to a tennis court. This gigantic surface is no accident of evolution: it represents the largest interface of contact between your body and the outside world. Much larger than your skin. Much more exposed than your lungs.
On this surface, more than five hundred bacterial species coexist in an equilibrium as fragile as it is sophisticated. Protective bacteria (Lactobacilli, Bifidobacteria) that line the mucous membrane, produce lactic acid, hydrogen peroxide, bacteriocins, and keep opportunistic species in the minority. Fermentation bacteria that degrade dietary fibers and produce short-chain fatty acids, notably butyrate, the preferred fuel of colon cells. Yeasts like Candida albicans, harmless as long as they remain under control, devastating when they take power.
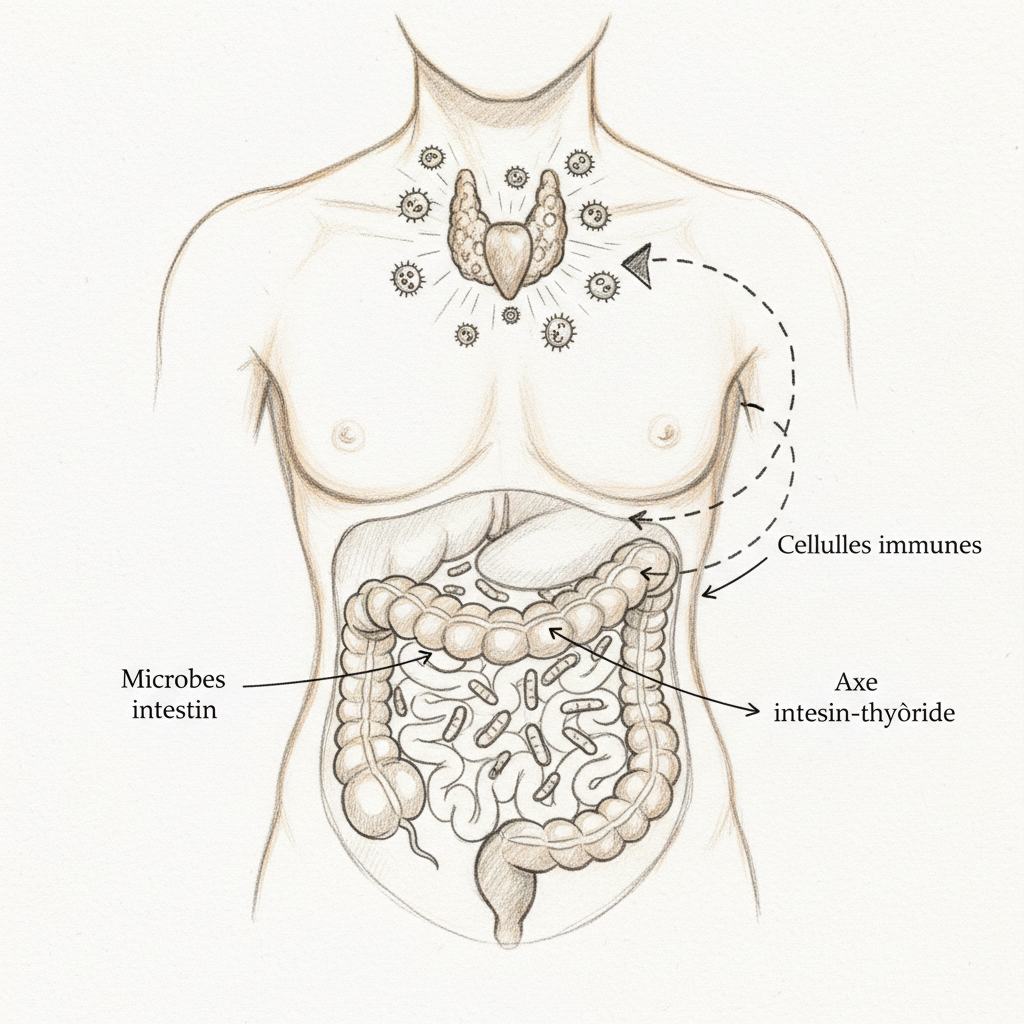
And in the middle of all this, the immune system. Seventy percent of your immune defenses reside in your intestine, within the GALT (Gut-Associated Lymphoid Tissue). It’s a figure I repeat often in consultation because it changes the perspective of most people. Your immunity doesn’t build itself in your bone marrow alone. It builds, regulates and modulates itself in your intestinal mucous membrane. Humoral immunity, that of B lymphocytes that manufacture antibodies, and cellular immunity, that of T lymphocytes that destroy infected or abnormal cells, both depend on the integrity of this ecosystem.
When this balance breaks down, when protective species decline and pathogenic or opportunistic species take over, we speak of dysbiosis. And dysbiosis isn’t simply “having bloating.” It’s an open door to practically all the chronic diseases I see coming through consultation. Autoimmunity, as I explain in my article on Hashimoto, often begins with an intestine that no longer performs its barrier function. Chronic fatigue, systemic inflammation, hormonal disorders: it all starts there. It’s the soil. If the soil is poisoned, nothing healthy can grow there.
The nine faces of dysbiosis
What makes dysbiosis so difficult to identify is that it doesn’t wear a single mask. It wears nine. And most patients who come to my office have never made the connection between their symptoms and their intestine, because these symptoms seem to have no relationship to each other.
The first face is the most obvious. Digestive troubles. Chronic bloating, excessive and foul-smelling gas (sign of intestinal fermentation or putrefaction), constipation-diarrhea alternation, heartburn, halitosis. Halitosis, that bad breath that nothing resolves, neither tooth brushing nor mouthwashes, is often the reflection of abnormal intestinal fermentation. The stomach ferments because the flora has lost its ability to properly break down food. Gases rise up. Breath becomes the mirror of the intestine.
The second face surprises more. Neurological troubles. Anxiety, fatigue, depression, insomnia, headaches. The link is direct nonetheless. Eighty percent of serotonin is produced in the intestine. Serotonin, that neurotransmitter that regulates your mood, your serenity, your sleep, your perception of pain. When the flora is disturbed, tryptophan production and its conversion to serotonin plummet. Anxiety sets in without apparent reason. Sleep degrades. Intestinal fungal infections, notably candidiasis, worsen the picture by producing mycotoxins that cross the blood-brain barrier. Acetaldehyde produced by Candida interferes with neurotransmitter synthesis. The liver overload that results amplifies fatigue. And chronic headaches, those migraines that nothing relieves, often find their origin in circulating mycotoxins and systemic inflammation of intestinal origin.
The third face is read on the skin. Chronic dermatoses. Adult acne, eczema, psoriasis, urticaria, rosacea. The skin is an organ of elimination. When the intestine no longer performs its barrier function, when the liver is saturated by toxins entering the circulation, the skin takes over. It eliminates through the surface what the intestine and liver can no longer manage in depth. Marchesseau taught this in his pamphlets: skin diseases are almost never diseases of the skin. They are intestinal diseases expressing themselves through the skin. Treating eczema with cortisone without looking at intestinal flora is painting a cracked wall.
The fourth face is that of recurrent infections. Otitis, sinusitis, bronchitis, repeated urinary tract infections. It’s exactly Nathalie’s story. The vicious circle is relentless: dysbiosis weakens mucosal immunity (drop in secretory IgA), which promotes infections. Infections are treated with antibiotics. Antibiotics worsen dysbiosis. Mucosal immunity collapses a bit more. And infections return, more frequent, more resistant. The patient spins in this wheel without anyone showing them the way out.
The fifth face is the most serious. Immunological troubles. Food and respiratory allergies, multiple intolerances, and especially autoimmune diseases. Hashimoto thyroiditis, Crohn’s disease, ulcerative colitis, rheumatoid polyarthritis. The mechanism is that which Seignalet described in his xeno-immune theory: dysbiosis alters intestinal permeability, bacterial and food macromolecules cross the barrier and enter the bloodstream, the immune system recognizes them as foreign, and through molecular mimicry, it ends up attacking body tissues that structurally resemble these intruding molecules.
The sixth face is that of chronic pain. Fibromyalgia, recurrent tendinitis, chronic low back pain. Seignalet classified fibromyalgia as a disease of encrassment: macromolecules that cross the leaky intestine deposit themselves in myocytes, tenocytes, neurons, creating slow and progressive intoxication of tissues. Fibromyalgia patients I accompany almost systematically present dysbiosis on stool culture. It’s not a coincidence.
The seventh face concerns women specifically. Recurrent urinary tract infections (the anatomical proximity between intestine and urogenital system facilitates bacterial translocation), dysmenorrhea, endometriosis, aggravated premenstrual syndrome. The intestinal flora plays a central role in estrogen metabolism via the estrobolome, that set of bacterial enzymes regulating estrogen reabsorption or elimination in the intestine. Dysbiosis disrupts the estrobolome, promotes estrogen recirculation, and fuels estrogen dominance underlying endometriosis, fibroids, severe PMS.
The eighth and ninth faces affect respectively children (colic, infant eczema, recurrent otitis, behavioral disorders, hyperactivity) and athletes (unexplained fatigue, performance decline, recurrent tendinitis, digestive troubles during exercise). In both cases, the common denominator is the same: an impoverished intestinal ecosystem that no longer fulfills its functions of digestion, absorption, immune protection and detoxification.
The three great destroyers
If dysbiosis is so widespread, it’s because our modern lifestyle attacks the intestine on all fronts at once. Three categories of aggressors stand out, and they often act synergistically.
Medications, first. Antibiotics are first on the list. A single course of broad-spectrum antibiotics can reduce microbiota diversity by thirty to fifty percent. Some protective species take six to twelve months to reconstitute. Others never return. And in the void left by destroyed commensal bacteria, Candida albicans proliferates, as I explain in detail in my article on the adrenal-candidiasis vicious circle. But antibiotics aren’t the only culprits. Proton pump inhibitors (PPI, such as omeprazole), prescribed like candy for acid reflux, reduce stomach acidity and allow pathogenic bacteria to colonize the small intestine (SIBO). Nonsteroidal anti-inflammatory drugs (NSAIDs, such as ibuprofen) directly increase intestinal permeability by damaging tight junctions. Corticosteroids depress mucosal immune function. And birth control pills decrease circulating zinc and weaken adrenal function, two factors that directly impact intestinal mucous membrane integrity.
Chronic stress, next. It’s a destroyer people underestimate because it’s invisible. Stress doesn’t puncture the intestine like a knife blow. It dries it out, slowly, insidiously, day after day. Chronically elevated cortisol reduces saliva production (first digestive enzyme), decreases hydrochloric acid secretion in the stomach (compromising protein digestion and food sterilization), slows pancreatic juice and bile secretion, and slows peristalsis. Result: food stagnates, ferments, putrefies. Pathogenic bacteria feed on this putrefaction. And cortisol, in parallel, directly increases intestinal permeability by degrading tight junction proteins. The gut-brain axis works both ways: stress destroys the flora, and the destroyed flora amplifies stress by reducing serotonin production and increasing pro-inflammatory cytokines. It’s a loop.
Modern diet, finally. Refined sugars and grain products selectively feed fermentation bacteria at the expense of protective bacteria. The gluten of modern wheat, with its toxic gliadins whose structure has been profoundly altered by genetic crossbreeding, directly attacks the mucous membrane by stimulating zonulin production, the protein that opens tight junctions. Conventional dairy products provide A1 casein, a protein whose incomplete digestion produces opioid peptides (casomorphins) that slow transit and maintain inflammation. And alcohol, even at “moderate” doses, alters the actin filaments of enterocytes, the cells forming the intestinal barrier. When actin is degraded, the enterocyte loses its structure, the barrier loosens, and macromolecules pass into the circulation. It’s leaky gut. The leaky gut syndrome, gateway to systemic inflammation and autoimmunity.
The four-phase restoration protocol
Restoring an intestinal ecosystem is gardener’s work. You don’t plant in poisoned soil. You start by removing toxins, you clean, you amend the earth, and only then do you plant. My protocol follows this logic in four phases. The order is fundamental. If you reverse the steps, you waste your time and money.
Phase 1: Eliminate aggressors. There’s no point rebuilding if bombs keep falling. The first action is dietary: elimination of refined sugars, gluten-containing grains (wheat, spelt, rye, barley), cow dairy products, alcohol, ultra-processed foods. It’s not a restrictive diet, it’s an act of protection. In parallel, reassess with the treating physician the necessity of PPIs (many cases of acid reflux are linked to low stomach acid, not excess acid, and PPIs worsen the problem), reduce NSAIDs to the bare minimum, and only take antibiotics when truly necessary. This phase lasts throughout the protocol and, ideally, becomes a lifestyle.
Phase 2: Sanitize the terrain. When dysbiosis has been established for a long time, when fungal candidiasis is suspected (sugar cravings, white tongue, recurrent fungal infections, brain fog), you must clean before rebuilding. Natural antimicrobials are remarkably effective when used correctly, that is, in rotation to prevent resistance. Grapefruit seed extract (GSE) at fifteen drops three times daily for two weeks, then berberine at five hundred milligrams twice daily for two weeks, then oregano essential oil (carvacrol and thymol, two powerful antifungal and antibacterial molecules) in enteric capsules for a maximum of ten days. Lactoferrin, a colostrum protein, chelates the iron that pathogenic bacteria need to proliferate. Caprylic acid (from coconut oil) and undecylenic acid specifically attack Candida fungal membranes. Pau d’arco (lapacho), tea tree and black walnut complete the arsenal when dysbiosis is severe. This phase lasts four to eight weeks, and the patient should be warned of possible Herxheimer reaction: when micro-organisms die in mass, they release their toxins, which can cause fatigue, headaches and temporary symptom worsening for a few days.
Phase 3: Repair the mucous membrane. This is the phase most people skip, and that’s why their probiotics don’t work. If the intestinal wall is porous, good bacteria have no healthy surface on which to establish themselves. L-glutamine is the star nutrient of this phase: four to eight grams daily, on an empty stomach, in a glass of water. Glutamine is the preferred fuel of enterocytes, the cells of the intestinal mucous membrane. It accelerates cell renewal and restores tight junctions. Zinc, at fifteen to thirty milligrams daily, is essential for mucosal regeneration and production of secretory IgA that line and protect the barrier. Retinol (active vitamin A, not beta-carotene) supports epithelial cell differentiation. Folic acid participates in rapid intestinal cell renewal. Butyrate, that short-chain fatty acid normally produced by good bacteria from fiber, can be provided as a supplement (six hundred milligrams daily) to directly feed colonocytes when the flora isn’t yet able to produce it itself. N-acetyl-glucosamine, a precursor of glycosaminoglycans composing the protective mucus, reinforces the mucus layer lining the intestine. Phospholipids (sunflower lecithin) restore the cell membranes of enterocytes. And omega-3 EPA/DHA, at minimum two grams daily, calm mucosal inflammation through the pathway of resolvins and protectins.
Polyphenols deserve special mention in this phase. Resveratrol, from grapes, and crocetine, from saffron, protect the mucous membrane against bacterial endotoxins (LPS) that maintain systemic inflammation. Ugurel and colleagues showed in 2016 that resveratrol significantly reduced the inflammatory response induced by LPS. Si and colleagues, the same year, demonstrated the synergistic effect of DHA and quercetin on protecting the intestinal barrier. Li et al. confirmed in 2017 that ginkgolide B attenuated LPS-induced damage to intestinal epithelial cells. Selenium (one hundred micrograms daily) and quercetin (five hundred milligrams daily) complete the antioxidant shield. Liver herbal teas (peppermint, milk thistle, artichoke, boldo, lemon balm) support the liver detoxification that works in tandem with the intestine to eliminate remobilized toxins. This phase lasts three to six months.
Phase 4: Reseed. It’s only now, on cleaned terrain and repaired mucous membrane, that probiotics make sense. Not before. Planting seeds in toxic soil is a waste of time. The strains that have demonstrated the most clinical efficacy are Lactobacillus (rhamnosus, acidophilus, plantarum) and Bifidobacterium (longum, breve, lactis), at a minimum of ten billion CFU daily, split into two doses away from meals, for a minimum of four to eight weeks. Saccharomyces boulardii, a non-pathogenic yeast, is particularly useful in cases of associated candidiasis as it occupies territory and prevents Candida from recolonizing. Prebiotics (FOS, GOS, inulin) selectively feed good bacteria, but must be introduced progressively as they can worsen bloating if the flora isn’t yet stabilized. And above all, above all: dietary diversity. Varied fibers, lacto-fermented vegetables (raw sauerkraut, kimchi, miso, fruit kefir), polyphenol-rich foods, this is what maintains microbial biodiversity in the long term. Probiotics in capsule form are a crutch. Diet is the real gardener.
What the numbers don’t say
There’s something I want to tell you that doesn’t fit into any table, any study, any meta-analysis. It’s raw clinical experience. In five years of consultations, I’ve seen patients that medicine had labeled “depressed” regain their joy of living in three months of intestinal protocol. I’ve seen women who had string of urinary tract infections never have another one after six months of flora restoration. I’ve seen “incurable” eczemas disappear as if someone had flipped a switch.
“The small intestine is a key piece whose good or poor functioning reverberates across many organs and tissues.” Jean Seignalet
Seignalet was right. The intestine is the key piece. Not one organ among others. The central piece around which everything else organizes itself. And when this piece malfunctions, the entire structure wavers. Symptoms vary from person to person (nine families, you remember), but the root is always the same: a broken ecosystem, a permeable barrier, a confused immune system.
Nathalie, the one who came for her urinary tract infections? We worked together for six months. Elimination of gluten and cow dairy products, the antimicrobial protocol in rotation, glutamine and zinc to repair the mucous membrane, targeted probiotics afterward. Her urinary tract infections spaced out in the second month, then disappeared in the fourth. Her hand eczema began regressing in the third month. Her anxiety melted away. Her fatigue lifted. It’s not magic. It’s physiology. When you repair the soil, plants regrow on their own.
Essential warning
I want to be clear on one point. Severe dysbiosis, that which accompanies autoimmune diseases, serious infections, malnutrition or unexplained weight loss, requires medical monitoring. Naturopathy doesn’t substitute for medicine. It complements it. Never stop an antibiotic course without medical advice, even if you’ve read this article and are convinced your antibiotics are worsening your dysbiosis. It might be true, but the acute infection they’re treating could be dangerous.
Autoimmune diseases, Crohn’s disease, ulcerative colitis always require coordination between doctor and naturopath. My role is to act on the terrain, to strengthen what medicine doesn’t look at. The doctor’s role is to monitor, diagnose, treat emergencies. The two approaches don’t oppose. They complement each other.
And now?
If you recognize yourself in several of the nine faces described in this article, there’s a strong chance your intestine needs attention. Not a “special flora” yogurt. Not a packet of probiotics bought at the pharmacy on impulse. A real protocol, structured, individualized, that respects the order of phases and takes the necessary time. Three to six months. That’s the price of reconstructing an ecosystem.
Naturopathy doesn’t offer miraculous solutions. It offers a reading of the terrain and patient, methodical, physiology-rooted accompaniment. If you want to deepen the links between intestine and thyroid, start with my article on thyroid and micronutrition. If it’s chronic fatigue that worries you, explore the fibromyalgia lead or the adrenal-candidiasis vicious circle. Everything is linked. Everything starts from the same place.
If you want personalized accompaniment, you can book a consultation.
To go further
- Intestinal dysbiosis: the 5 profiles sabotaging your thyroid
- Digestion and microbiota: what metagenomics analysis reveals about your gut
- Chronic constipation: the 7 causes your doctor isn’t looking for
- Intestinal microbiota: the hidden organ governing your health
Sources
- Kousmine, Catherine. Soyez bien dans votre assiette jusqu’à 80 ans et plus. Tchou, 1980.
- Seignalet, Jean. L’alimentation ou la troisième médecine. 5e éd. François-Xavier de Guibert, 2004.
- Marchesseau, Pierre-Valentin. Fascicules de naturopathie (1950-1980).
- Ugurel, E. et al. “Resveratrol reduces LPS-induced inflammatory response in human monocytes.” Journal of Medicinal Food, 2016.
- Si, H. et al. “DHA and quercetin synergistically protect intestinal barrier function.” Journal of Nutritional Biochemistry, 2016.
- Li, W. et al. “Ginkgolide B attenuates LPS-induced intestinal epithelial cell injury.” International Immunopharmacology, 2017.
You can book a consultation for a complete intestinal assessment. I see patients in Paris and via video throughout France.



Laisser un commentaire
Sois le premier à commenter cet article.