When Marie arrived for her consultation, she placed on the table a medical file as thick as a phone book. Three endocrinologists, two general practitioners, one rheumatologist. Unanimous diagnosis: hypothyroidism. Treatment: Levothyrox 75 micrograms. Prognosis: for life. What no one had sought, however, was why her thyroid had slowed down. Why this thirty-eight-year-old woman, athletic, with no particular medical history, had started shivering in June, losing her hair by the handful and gaining six kilos in four months. The word “hypothyroidism” had closed the investigation before it even began.
After more than three hundred consultations related to the thyroid, I can state this observation with certainty: hypothyroidism is almost never a final diagnosis. It’s a signal. A warning light on the dashboard of an organism suffering upstream. And as long as you don’t find the cause, you’re just repainting the warning light.
Dr. Pache wrote: “All disease is an appointment and not an accident; disease is prepared long in advance by failures of hygiene.” This sentence alone could summarize my daily practice in the clinic. Hypothyroidism doesn’t come out of nowhere. It is prepared, constructed, fed by a set of imbalances that converge toward the thyroid like tributaries toward a river. If you want to understand the basics of terrain in naturopathy, I invite you to read the basics of naturopathy before continuing.
Why “hypothyroidism” is not a diagnosis
The word “hypothyroidism” describes a state: the thyroid doesn’t produce enough hormones. But it says nothing about the reason for this state. It’s like telling a patient they have a fever without looking for the infection. Fever is not the disease; it’s the body’s response to a problem. Hypothyroidism works exactly the same way.
Dr. Benoît Claeys explains this in “En finir avec l’hypothyroïdie” with remarkable clarity. He distinguishes several levels. Primary hypothyroidism affects the gland itself: either through autoimmunity (Hashimoto), or through lack of nutritional cofactors (iodine, tyrosine, selenium, zinc, iron), or through a defect in converting T4 to T3, or through resistance of cell receptors to T3. Secondary hypothyroidism comes from the pituitary, which doesn’t produce enough TSH to stimulate the thyroid. Tertiary hypothyroidism comes from the hypothalamus, which doesn’t produce enough TRH to stimulate the pituitary. And congenital hypothyroidism is present from birth, often linked to maternal iodine deficiency during pregnancy.
Most doctors stop at the first level. High TSH, low T4, here’s your prescription. But even within primary hypothyroidism, the causes are multiple and each requires a different approach. Hashimoto is not treated like iodine deficiency. A hepatic conversion defect isn’t corrected with Levothyrox. And cellular resistance linked to excess estrogen requires work on hormonal balance, not on the thyroid itself.
This confusion between the signal and the cause explains why so many thyroid patients continue to suffer despite their treatment. Their warning light is off (TSH returns to normal), but the engine keeps heating up.
The five upstream causes

In my consultations, I have identified five major categories of causes that fuel hypothyroidism. They are not mutually exclusive. On the contrary, they combine and worsen each other, creating a network of imbalances of which the thyroid is only the point of convergence.
The first cause, and the most frequent in my clinic, is deficiency in nutritional cofactors. The thyroid is a hormone production factory that operates with precise raw materials: iodine, tyrosine, selenium, zinc, iron, magnesium, vitamins A, D, E, B1, B2, B3, B6, B12, copper, manganese, molybdenum. If even one of these elements is missing, the production chain is compromised. Dr. Claeys estimates that more than ninety percent of his thyroid patients have a clear zinc deficiency. The ENNS study shows that eighty percent of French people are insufficient in vitamin D. The ferritin of most women I see is below 30 ng/mL when the functional goal is between 50 and 80. I detailed these cofactors in my article on thyroid and micronutrition.
The second cause is an overloaded liver. The liver ensures approximately sixty percent of the conversion of T4 (inactive pro-hormone) to T3 (active hormone). It synthesizes TBG, the protein that transports thyroid hormones in the blood. It metabolizes excess estrogen that blocks the thyroid. And it regulates cholesterol via HMG-CoA reductase, an enzyme directly activated by T3. A liver clogged by overly rich food, alcohol, medications, stress, or environmental toxins becomes incapable of performing these functions. How many patients are prescribed statins for cholesterol that is only the reflection of a suffering thyroid? Non-alcoholic fatty liver disease, this “fatty liver” found in one out of four French people, is both a cause and consequence of hypothyroidism.
The third cause is intestinal permeability. The small intestine is the second site of T4 to T3 conversion after the liver (approximately twenty percent). But most importantly, a porous intestine creates two major problems. First, it absorbs nutrients poorly, which worsens the deficiencies described above. Second, it lets through the circulation food and bacterial peptides that can trigger an autoimmune reaction against the thyroid, the mechanism described by Seignalet in Hashimoto. Intestinal dysbiosis, food intolerances (gluten, casein), chronic candidiasis, and regular use of anti-inflammatory drugs are all factors that weaken this barrier.
The fourth cause is adrenal exhaustion. Cortisol, the stress hormone, maintains an intimate relationship with the thyroid. When the adrenals are overworked by chronic stress, elevated cortisol directly inhibits the conversion of T4 to active T3 and promotes the production of reverse T3, an inactive form that blocks cell receptors. Dr. Hertoghe emphasizes this point in his training: the adrenals must always be evaluated before treating the thyroid. Giving thyroid hormones to a patient whose adrenals are exhausted is like whipping an exhausted horse. The theft of pregnenolone, the mechanism by which the body sacrifices the production of progesterone and DHEA in favor of cortisol, is a classic in thyroid consultations.
The fifth cause is exposure to xenobiotics. According to the EFSA, one hundred and one pesticides out of two hundred and eighty-seven evaluated affect the thyroid. Heavy metals (mercury from dental fillings, lead, cadmium), fluoride (in tap water and toothpaste), endocrine disruptors (phthalates, bisphenols, PCBs, dioxins) disrupt the synthesis, metabolism and transport of thyroid hormones. If you’re still cooking with utensils that release toxic substances, see my article on endocrine disruptors in the kitchen.
The law of the limiting factor

Chemist Justus von Liebig formulated in the nineteenth century a simple law that revolutionizes the understanding of the thyroid: the growth of a plant is determined not by the total quantity of resources available, but by the rarest resource. Liebig illustrated this law with a barrel whose staves are of unequal lengths. The water level in the barrel is determined by the shortest stave, regardless of the height of the others.
Applied to the thyroid, this law illuminates a phenomenon I constantly observe in consultations. A patient may have sufficient intake of iodine, zinc, magnesium, vitamin D, but if her selenium is collapsed, the entire T4 to T3 conversion chain is blocked. The thyroid produces its T4, but the selenoproteins that ensure the conversion cannot function. Result: functional hypothyroidism despite normal hormone production.
I’ve seen cases where simply correcting iron (ferritin was at 12 ng/mL) was enough to normalize the entire thyroid panel in three months. I’ve seen others where it was selenium, or vitamin D, or magnesium. In each case, a single limiting factor kept the patient in a state of hypothyroidism that years of Levothyrox had not corrected. Because Levothyrox provides T4, but it doesn’t provide the cofactors necessary for its conversion.
Dr. Didier Cosserat uses an enlightening image in his works. He compares the thyroid to a washing machine. Levothyrox is like putting laundry in the machine. But if the machine has no water (iron), no detergent (selenium), no electricity (magnesium), and no drain hose (the liver), the laundry comes out as dirty as before. Hormone replacement therapy is essential when thyroid tissue is destroyed (advanced Hashimoto, thyroidectomy), but in all other cases, the priority is to find and correct the limiting factor.
This approach is what makes me say that hypothyroidism is a symptom and not a diagnosis. When you identify the limiting factor, when you correct the shortest stave of the barrel, the water naturally rises. The thyroid starts functioning again, not because you forced it with exogenous hormones, but because you gave it back the conditions necessary for its functioning.
Evaluate your thyroid

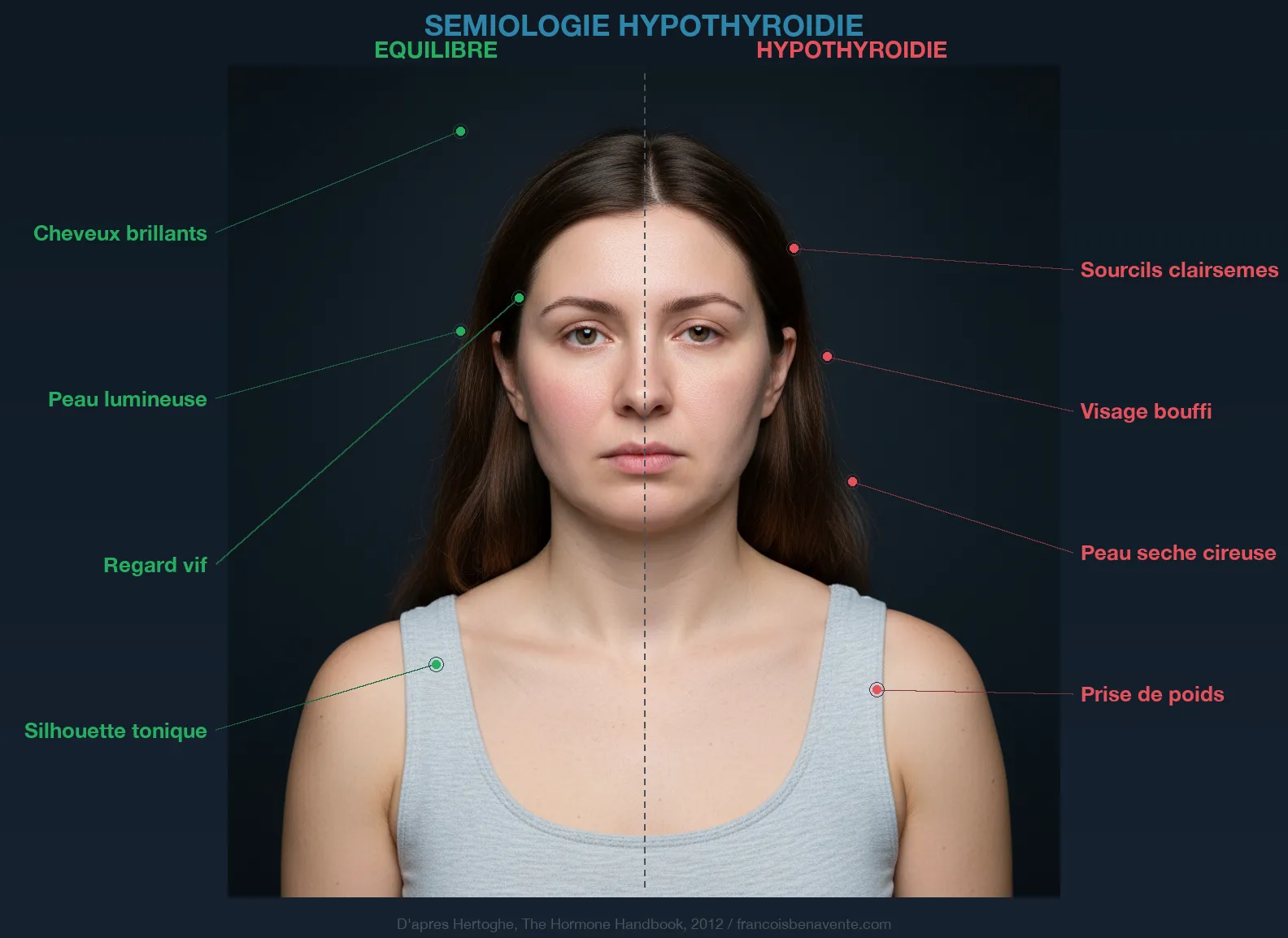
Dr. Eugène Hertoghe published as early as 1880 a clinical examination of hypothyroidism based on observation and questioning. His great-grandson, Dr. Thierry Hertoghe, continued this work in his Hormone Handbook with one hundred and seven registered symptoms. The Colorado Thyroid Disease Prevalence Study, conducted on more than twenty-five thousand participants, quantified the nine main symptoms.
The self-assessment I propose in consultations unfolds in three stages. The first stage explores family history: thyroid in siblings, parents, grandparents. A hereditary terrain of hypothyroidism exists, even though it is never a fatality. The second stage looks for signs that appeared from childhood: flat feet, overlapping teeth, height below average, persistent cradle cap. These signs reflect a thyroid that could not develop properly, often due to iodine deficiency in the mother during pregnancy. The third stage evaluates signs that appeared after puberty: excessive coldness, disproportionate fatigue, hair loss, unexplained weight gain, chronic constipation, dry skin, brain fog, depression, loss of the outer third of the eyebrows (the famous Hertoghe sign), bradycardia.
If your score exceeds ten points on this scale, a complete thyroid panel is justified. Beyond thirty points, treatment becomes necessary. But be careful: a high score doesn’t automatically mean your thyroid is the problem. Dr. Hertoghe himself emphasizes that certain deficiencies in cortisol, vitamin D, iron, zinc, or B vitamins give a clinical picture almost identical to hypothyroidism. This is precisely why the diagnosis must go beyond simple TSH measurement.
Basal body temperature remains a valuable and free clinical tool. Take your temperature under your tongue for three consecutive mornings, upon waking, before getting up. Below 36.3 degrees Celsius in the morning according to Dr. Mouton, the thyroid hypothesis is serious. Below 36 degrees, it’s almost certain. Want to go further? The Claeys questionnaire is available on my website.
The difficult path
The Scientific Council of Luxembourg produced a decision tree that I regularly use in consultations to explain the diagnostic path to my patients. It starts with TSH. If your TSH is less than 4 mU/L, the doctor stops there. Game over. Yet, according to Dr. Claeys, physiological norms are between 0.25 and 1.3 mU/L. A TSH of 3.5, “within normal range” for your lab, may already reflect a suffering thyroid.
If TSH is elevated, the doctor continues with free T4. But as Claeys points out, measuring TSH and T4 really amounts to measuring the same thing twice, since TSH only rises when T4 drops. It’s like checking that your car is out of fuel by looking at the gauge AND the level in the tank. The information is the same.
The real question is elsewhere: what does your body do with this T4? Does it convert it correctly to active T3? This is where the standard panel stops and the naturopathic investigation begins. According to Claeys, the most reliable way to diagnose hypothyroidism is to measure the T3/TBG ratio. When T3 is lacking, the body produces more carrier proteins (TBG). A T3/TBG ratio below 0.04 allows you to strongly suspect functional hypothyroidism, even if TSH and T4 seem normal.
And sometimes, even this ratio is not enough. A study published in the Lancet by Dr. J. Hertoghe’s team on eight hundred and twenty-two hypothyroid patients demonstrated the superiority of urine analysis over blood tests for diagnosis. A blood test is a bit like a bank statement for the day: it gives you a snapshot at one moment in time, but it says nothing about the rest of the month. Since the thyroid has a rhythm that varies from one hour to the next, twenty-four-hour urine analysis gives a much more accurate picture.
If the panel reveals hypothyroidism, four major leads must be explored. Either the thyroid doesn’t produce enough T4 (lack of basic building blocks). Or the T4 to T3 conversion isn’t happening correctly (liver, selenium, iron). Or T4 is converted to reverse T3 instead of active T3 (stress, inflammation, heavy metals). Or T3 cannot penetrate cells (vitamin D deficiency, omega-3 deficiency, excess estrogen, colloidal waste). The answer to these questions determines the treatment. And in each case, the answer points to a cause upstream of the thyroid, not the thyroid itself.
What I propose in consultation
My approach in thyroid consultation is simple in principle and demanding in implementation. It consists of following the thread of the ball rather than cutting the knot.
The first step is a complete functional assessment: TSH, free T3, free T4, reverse T3, free T3/reverse T3 ratio, antibodies (anti-TPO, anti-Tg, anti-TSH receptors), plus cofactors (selenium, zinc, copper, ferritin, vitamin D, red blood cell magnesium, homocysteine, B12, folates). This assessment far exceeds what a standard general practitioner prescribes, but it’s essential to understand at which level the problem is located.
The second step is identifying the limiting factor or factors. The biological assessment, crossed with the medical history, clinical examination (basal temperature, Hertoghe sign, skin condition, transit, weight) and the Hertoghe questionnaire, allows you to draw a map of imbalances. In Marie’s case, which I mentioned in the introduction, the limiting factors were a collapsed ferritin (14 ng/mL) and an overloaded liver (elevated gamma-GT, ASAT greater than ALAT). Her thyroid had no problem. Her liver and iron did.
The third step is targeted correction. You don’t supplement everything at once. You correct the most limiting factor first, you reevaluate at six weeks, you adjust. Adrenals before thyroid. Iron and selenium before iodine. Intestine before supplements (otherwise malabsorption cancels out the effect of supplementation). It’s precision work, not bombardment.
The fourth step is monitoring the terrain as a whole. The thyroid doesn’t live in isolation. It depends on the liver, adrenals, intestine, hormonal balance, sleep, movement, stress management. Correcting a deficiency without correcting the lifestyle that created it is like filling a leaky bucket. This is why each consultation includes a dietary component (chrono-nutrition, food combinations, cooking quality), an emotional component (stress, sleep, repressed emotions), and a physical component (movement, hydrotherapy, cold exposure).
Want to go deeper into each of these dimensions? My article on thyroid and micronutrition details the seven essential cofactors. The article on Hashimoto explores the autoimmune mechanism. And the one on zinc explains why this mineral is so often the limiting factor in thyroid patients.
Restoring the thyroid’s conditions for functioning
Back to Marie. Six months after our first consultation, her ferritin had risen to 52 ng/mL. Her liver had been drained with a protocol of cellulose dinners, rosemary-ginger decoctions and alcohol elimination. Her free T3, which had been low despite Levothyrox, had normalized. Her endocrinologist had even reduced the dosage. She was no longer cold all the time. Her hair had stopped falling out. She had regained the energy to play with her children in the evening instead of collapsing on the sofa at six pm.
Nothing spectacular in this protocol. No miracle molecule. No revolutionary discovery. Just the identification of a limiting factor and its methodical correction. Just the replacement of the shortest stave in Liebig’s barrel.
Marchesseau wrote: “The naturopath doesn’t treat disease; he corrects the terrain that allowed disease to establish itself.” Hypothyroidism perfectly embodies this philosophy. It’s not the thyroid that needs to be treated first. It’s the terrain that brought it to its knees.
If you recognize yourself in what you’ve just read, if you’ve been taking Levothyrox for months or years without real improvement, if your TSH is “within normal range” but you feel exhausted, cold, foggy, the question isn’t “is my thyroid working poorly?” but “why is it working poorly?”. The answer is rarely found in the thyroid itself. It’s found in your liver, intestine, adrenals, diet, environment. It’s found in the limiting factor that no one looked for.
If you want personalized support, you can book a consultation appointment.
To go further
- Thyroid: the 7 nutrients your endocrinologist never tests
- Carnitine and thyroid: the molecule no one tests
- Low ferritin and hair loss: the connection your doctor ignores
- The Hertoghe method: hormones, micronutrition and terrain medicine
Want to assess your status? Take the free vitality toxemia questionnaire in 2 minutes.
Sources
- Hertoghe, Thierry. The Hormone Handbook. 2nd ed. Luxembourg: International Medical Books, 2012.
- Marchesseau, Pierre-Valentin. Founder of French naturopathy, author of numerous pamphlets (1950-1980).
- Mouton, Georges. Digestive Ecology. Marco Pietteur, 2004.
- Vernay, M. et al. “Vitamin D Status in the French Adult Population (ENNS, 2006-2007).” Urology Annals 4, no. 3 (2012): 163-172.
To sleep well, support serotonin and correct zinc deficiencies that sabotage your T4 to T3 conversion, see the dedicated articles. And if you need personalized support to identify your limiting factor, you can book a consultation appointment.
Based in Paris, I consult via video throughout France. Quality thyroid supplementation is available at Sunday Natural (-10% with code FRANCOIS10).
Healthy recipe: Immunity juice with turmeric-ginger: This juice supports the thyroid and immunity.






Laisser un commentaire
Sois le premier à commenter cet article.