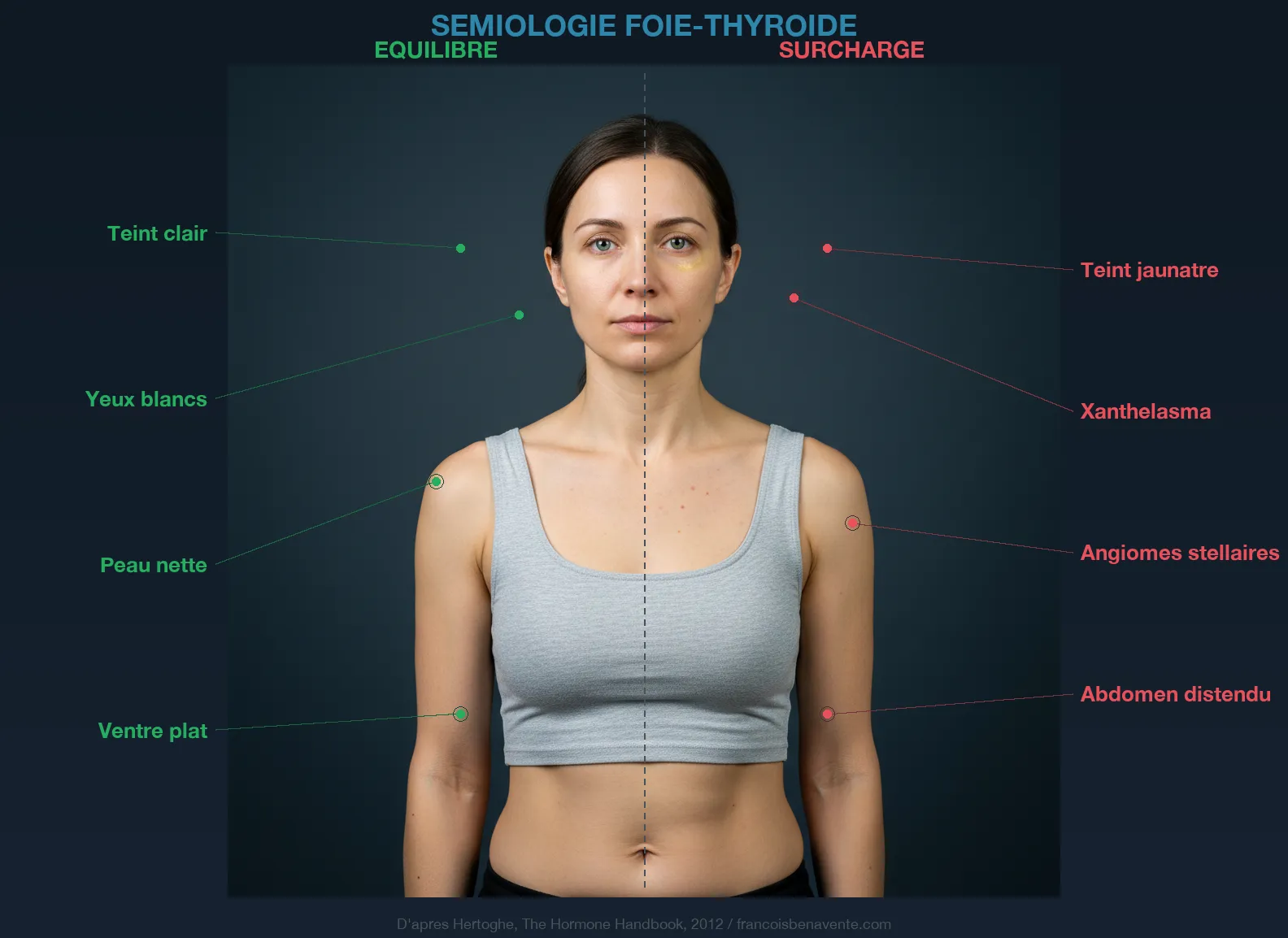
How many patients are prescribed statins for a cholesterol that is merely the reflection of a suffering thyroid? The question has haunted me since my first consultations. Because the pattern repeats, again and again: a person arrives with a “imbalanced” lipid panel, an anti-cholesterol treatment prescribed immediately afterwards, and fatigue that worsens. No one told them that their liver and thyroid are two organs that function in tandem. That if one slows down, the other collapses. And that rising cholesterol is not a disease, but a signal.
The liver converts sixty percent of T4 into active T3. I repeat this often because this figure changes everything. Your liver is not just a detoxification organ. It is the primary site of transformation of your inactive thyroid prohormone (T4) into active hormone (T3). If your liver is engorged, overloaded, fatty, inflamed, this conversion does not happen. You can take all the Levothyrox in the world, it brings you T4. But if your liver does not convert it, it serves no purpose.
The bidirectional relationship
To understand why the liver and thyroid form an inseparable duo, you must grasp that their relationship functions in both directions.

In the thyroid-to-liver direction, active T3 directly stimulates hepatic function. It activates HMG-CoA reductase, the key enzyme in cholesterol metabolism. It stimulates bile secretion. It accelerates beta-oxidation of fatty acids in hepatocytes. It promotes the synthesis of TBG (Thyroid Binding Globulin), the protein that transports thyroid hormones in the blood. And it participates in the metabolization of estrogens through hepatic glucuronidation and sulfation pathways.
In the liver-to-thyroid direction, the liver ensures most of the T4 to T3 conversion through deiodinase enzymes (primarily DIO1). It produces TBG which transports thyroid hormones to target cells. It metabolizes excess estrogens which, when they accumulate, increase TBG and sequester thyroid hormones. It synthesizes transport proteins for vitamin A and retinol, cofactors of thyroid synthesis. And it detoxifies xenobiotics that disrupt thyroid function (pesticides, heavy metals, endocrine disruptors).
When one of the two organs slows down, the other immediately suffers the consequences. Hypothyroidism slows the liver. A slowed liver converts less T4 to T3. Less T3 worsens hypothyroidism. It is a vicious circle as insidious as the one I described between the thyroid and digestion.
The cholesterol trap
This is probably the most frequent and most costly trap in thyroid medicine. A hypothyroid patient presents with elevated LDL cholesterol. The doctor, conditioned by cardiovascular recommendations, prescribes a statin. Cholesterol drops on paper, the doctor is satisfied, the patient remains fatigued.

What was not understood is that elevated cholesterol in a hypothyroid person is not the same thing as primary hypercholesterolemia. In hypothyroidism, HMG-CoA reductase runs slowly because it lacks T3 to activate it. The liver no longer properly transforms cholesterol into bile acids. The hepatic clearance of LDL particles is reduced. Hepatic LDL receptors are under-expressed. The result on the blood test is the same (elevated LDL), but the mechanism is completely different. So the treatment should be too.
Statins, by inhibiting HMG-CoA reductase, worsen the underlying problem: they reduce cholesterol production (which is also the precursor to all steroid hormones, including cortisol, progesterone and DHEA) and they deplete coenzyme Q10, a mitochondrial antioxidant that the thyroid needs for its own protection against oxidative stress.
In consultation, when a patient arrives with elevated cholesterol and signs of hypothyroidism, my first reaction is never to reduce cholesterol. It is to check the thyroid. If TSH is above 2 mU/L, if free T3 is low, if cofactors (selenium, zinc, iron, vitamin D) are deficient, cholesterol is a symptom, not a disease. And the treatment is to correct the thyroid, not to block a hepatic enzyme.
I have seen patients whose total cholesterol dropped from 2.80 g/L to 2.20 g/L in three months, simply by correcting a selenium deficiency and optimizing T4-T3 conversion. No statin. No fat-free diet. Just the right T3 that restarts HMG-CoA reductase. If you want to understand why hypothyroidism is a symptom and not a diagnosis, that article will give you the conceptual framework.
Hepatic steatosis: the thyroid fatty liver
Non-alcoholic fatty liver disease (NAFLD) affects one quarter of the Western population. This “fatty liver” unrelated to alcohol is an accumulation of triglycerides in hepatic cells. In hypothyroidism, the risk of steatosis is considerably increased, and for good reason: T3 stimulates beta-oxidation of fatty acids in the liver. When T3 is lacking, fatty acids are not burned and accumulate in hepatocytes.
Steatosis creates its own problems. A fatty liver is an inflamed liver. Hepatic inflammation disrupts the pathways of T4 to T3 conversion. Pro-inflammatory cytokines (TNF-alpha, IL-6) directly inhibit deiodinases. The result is a worsening of hypothyroidism by the liver itself that should correct it.
Resistance to insulin is the third corner of this infernal triangle. Hypothyroidism promotes insulin resistance. Insulin resistance promotes hepatic fat storage. Fatty liver worsens insulin resistance. And the loop closes. This is why I never separate the thyroid question from the overall metabolic question, as I explain in my article on thyroid and weight.
Estrogens and TBG
TBG (Thyroid Binding Globulin) is the main transport protein for thyroid hormones in the blood. Approximately ninety-nine percent of circulating T4 and T3 are bound to transport proteins, mainly TBG. Only the free fraction (free T3, free T4) is biologically active and capable of penetrating cells.
Estrogens increase hepatic TBG production. More estrogens means more TBG, which means more thyroid hormones sequestered and less free T3 available for cells. This is the mechanism by which oral contraceptives, hormone replacement therapy for menopause (HRT), pregnancy and relative hyperestrogenism (premenstrual syndrome, endometriosis, PCOS) worsen functional hypothyroidism.
The liver is the primary site of estrogen detoxification. Hepatic glucuronidation and sulfation pathways transform active estrogens into inactive metabolites that are excreted in bile and then eliminated through stool. An overloaded liver does not properly detoxify estrogens, creating a relative excess that increases TBG and sequesters thyroid hormones. The circle is complete.
Women suffering from painful periods, endometriosis or PCOS are particularly exposed to this mechanism. Their relative excess of estrogens overloads the liver while blocking the thyroid via TBG.
Hepatic drainage: the forgotten key

In consultation, I consider hepatic drainage as a prerequisite to any thyroid supplementation. Supplementing with selenium, zinc, iron without first lightening the liver is like pouring clean water into a clogged pipe. The nutrient does not circulate.
Food is the first lever. Cellulose dinners (abundant green vegetables, vegetable soups, mixed salads) two to three evenings per week lighten nocturnal hepatic work, the period when the liver ensures most of the hormonal conversion. Fresh vegetable juices in the morning (carrot, beet, celery, ginger, turmeric) made with a juice extractor provide the micronutrients and enzymes necessary for detoxification pathways without overloading digestion.
Cruciferous vegetables (broccoli, cauliflower, kale, Brussels sprouts) are precious allies. They contain indole-3-carbinol (I3C) and sulforaphane which activate hepatic detoxification pathways for estrogens and xenobiotics. However, be careful to consume them cooked (not raw in excess), because their goitrogenic compounds (thiocyanates) can inhibit iodine uptake by the thyroid when consumed raw in large quantities. Gentle cooking preserves nutrients while deactivating goitrogens.
Hepatic plants are the second lever. Milk thistle (silymarin) protects hepatocytes against oxidative stress and stimulates hepatic regeneration. Artichoke (cynarin) stimulates bile secretion and facilitates fat digestion. Rosemary (rosmarinic acid) is a powerful hepatic antioxidant. Dandelion (root) is a cholagogue and gentle diuretic. Ginger-rosemary decoction in the morning on an empty stomach is a classic in my consultation prescriptions.
Hydration is the third lever. The liver needs water to function. Dehydration thickens bile, slows detoxification pathways and compromises portal circulation. Thirty milliliters per kilogram of body weight is Dr. Batmanghelidj’s recommendation.
Alcohol is the fourth point, by omission. Alcohol blocks the hepatic enzyme that metabolizes estrogens. Even “moderate” consumption (one to two drinks per day) can be enough to saturate glucuronidation pathways and maintain relative hyperestrogenism. In thyroid terrain, the suppression or drastic reduction of alcohol is a powerful and underestimated lever.
The hepatic assessment of the thyroid patient
A complete hepatic assessment should be part of any serious thyroid assessment. Transaminases (AST, ALT) reveal hepatocyte suffering. An AST/ALT ratio greater than 1 points towards steatosis. Gamma-GT is a marker of hepatic overload (not only alcoholic). Alkaline phosphatase reflects biliary function. The complete lipid panel (total cholesterol, LDL, HDL, triglycerides) should never be interpreted without verifying thyroid function.
Bilirubin, often overlooked, is an underestimated marker. Elevated total bilirubin can reflect hepatic congestion or hemolysis. Albumin, synthesized by the liver, reflects the capacity of hepatic protein synthesis. Homocysteine, although primarily a methylation marker, is partly metabolized by the liver and its elevation can reflect both B12/folate deficiency and hepatic overload.
Dr. Cosserat recommends systematically testing cholesterol in every hypothyroid patient and never prescribing a statin before correcting thyroid function. If cholesterol normalizes with thyroid correction (which is the case in the majority of hypothyroidism), the statin was not necessary. If cholesterol remains elevated despite optimized thyroid function, then and only then does the question of specific treatment arise.
To deepen your knowledge of the 7 essential thyroid nutrients and understand the autoimmune mechanism of Hashimoto, consult the dedicated articles. The liver is at the crossroads of all these issues. This is why, in naturopathy, we often say that the liver is the first organ to cleanse and the last to forget.
To sleep well and allow your liver to perform its nighttime conversion functions, sleep is fundamental. The liver reaches its peak activity between one and three in the morning according to Chinese chronobiology. If you systematically wake up at this hour, the hepatic pathway is worth exploring.
If you need personalized support to untangle the relationship between your liver and your thyroid, you can book a consultation. Based in Paris, I consult via video throughout France. For hepatic and thyroid supplementation, Sunday Natural (-10% with code FRANCOIS10).
Do you want to assess your status? Take the free Claeys thyroid questionnaire in 2 minutes.
If you want personalized support, you can book a consultation.
To go further
- Carnitine and thyroid: the molecule that no one tests
- Cholesterol and cardiovascular disease: the real culprits your cardiologist is not looking for
- Low ferritin and hair loss: the link your doctor ignores
- Hypothyroidism is a symptom, not a diagnosis
Healthy recipe: Hepatic detox juice: This juice supports the liver, which is essential for the thyroid.





Laisser un commentaire
Sois le premier à commenter cet article.