Claire is forty-four years old. She has been taking Levothyrox for two years. Her endocrinologist adjusts the dosage every three months, sometimes up, sometimes down, never finding the right balance. She is always tired. Not ordinary fatigue, the kind you feel after a bad night. No, a deep, visceral fatigue that doesn’t go away with sleep or vacation. In the morning, she needs two coffees to function. Around three o’clock in the afternoon, she collapses. In the evening, paradoxically, she wakes up a bit, but sleep eludes her until two in the morning. When I asked her how long this had been going on, she looked at me with that expression I know well, the one of patients who have stopped hoping for an answer, and she said: “Since forever. Or almost.”
Her file contained three impeccable thyroid assessments. TSH within normal range. Free T4 adequate. No antibodies. On paper, Claire was fine. But nobody had measured her salivary cortisol. Nobody had looked at her adrenals. And nobody had explained to her that her problem might not be thyroid, but adrenal. That her thyroid was running slow not because it was sick, but because her adrenals, exhausted by years of chronic stress, had diverted the entire hormonal machinery to their benefit.
Dr Didier Cosserat writes in his work on adrenal fatigue: “Adrenal fatigue is perhaps the most frequent cause of thyroid insufficiency, whether clinical or subclinical, and yet the most often overlooked.” This sentence resonates in my office almost every week. Because out of more than three hundred thyroid consultations, I estimate that one third of the patients I see don’t suffer from a thyroid problem in the strict sense. They suffer from an adrenal problem that disguises itself as hypothyroidism.
If you want to first understand how the thyroid works globally and its nutritional cofactors, start with my article on the thyroid and micronutrition. If you want to understand why hypothyroidism is not a diagnosis but a symptom, read this article. Here, we’re going to dive into the triangle of cortisol, adrenals, and thyroid. And above all, we’re going to talk about the order in which to treat these two systems, because the order is everything.
The triangle nobody explains to you
To understand why the adrenals and thyroid are so intimately linked, you need to go back to a brain structure that orchestrates both: the hypothalamus. The hypothalamus is the hormonal conductor of your body. It pilots two axes in parallel. The hypothalamic-pituitary-thyroid axis (HPT) controls your thyroid via TRH then TSH. The hypothalamic-pituitary-adrenal axis (HPA) controls your adrenals via CRH then ACTH. These two axes share the same starting point. They use the same feedback circuits. And when one accelerates, the other pays the price.
Cortisol, the hormone produced by the adrenals in response to stress, is at the center of this interaction. In physiological quantities, cortisol is essential. It maintains blood sugar, regulates inflammation, allows you to get out of bed in the morning. But when stress becomes chronic, when cortisol stays elevated day after day, week after week, the damage begins. Excess cortisol directly inhibits TSH production by the pituitary. Less TSH means less thyroid stimulation. Dr Hertoghe emphasizes this point in his training: a patient in chronic hypercortisolism almost always has low or low-normal TSH, not because their thyroid is fine, but because the pituitary is muzzled by cortisol.
But cortisol doesn’t stop there. It also blocks the conversion of T4 to active T3 at the liver and peripheral tissues level. The liver, let’s remind ourselves, ensures about sixty percent of this conversion. I detailed this liver mechanism in my article on thyroid and liver. Under the effect of chronic cortisol, the deiodinase enzymes that ensure this conversion are inhibited. T4 is then redirected to an alternative pathway: reverse T3.
Reverse T3, this hormone that steals your life
Reverse T3 is perhaps the most misunderstood concept in all of endocrinology. And yet, it’s one of the most important for anyone suffering from unexplained chronic fatigue. Reverse T3 is a mirror image of active T3. Chemically, it’s the same molecule, but reversed. It binds to the same cellular receptors as active T3, except it doesn’t activate them. It blocks them. Imagine a key that goes into the lock but doesn’t turn, and prevents the right key from going in. That’s exactly what reverse T3 does.

In normal situations, your body produces some reverse T3. It’s a regulation mechanism, a physiological brake. But under chronic stress, under inflammation, in the presence of heavy metals or chronic diseases, the balance shifts. The body converts more and more T4 to reverse T3 instead of active T3. It’s a survival strategy: facing danger, your body slows your metabolism to conserve energy. During periods of famine, serious illness, or immediate danger, this is intelligent. But when the “danger” is a noisy open office, a toxic boss, too-short nights, permanent mental burden, and a mortgage that weighs you down, this survival mechanism turns against you.
The diagnostic trap is formidable. Your TSH can be normal. Your free T4 can be normal. Even your free T3 can seem acceptable. But if your reverse T3 is high, the ratio of active T3 to reverse T3 collapses, and your cells are in hypothyroidism while your blood test says the opposite. Dr Lam, a specialist in adrenal fatigue, calls this the “normal test syndrome.” You have all the symptoms of hypothyroidism, you feel shut down, slowed, cold-sensitive, brain-fogged, but your doctor looks at the numbers and tells you everything is fine. Some patients end up seeing a psychiatrist when the problem is purely hormonal.
This phenomenon of reverse T3 dominance has a characteristic that makes it even more insidious: it persists even after cortisol has normalized. Reverse T3 has a longer half-life than active T3. It accumulates in tissues. Cellular receptors, saturated by reverse T3, take time to “unclog.” This is why some patients, even after leaving a stressful environment, take months to recover. Cortisol has gone back down, but the damage persists.
The pregnenolone steal, or how stress diverts your hormones
There is an even deeper mechanism that explains why chronic stress devastates the hormonal system as a whole. This mechanism has a telling name: the pregnenolone steal. Or “pregnenolone steal” in English.

Pregnenolone is the mother molecule. It is made from cholesterol in the mitochondria, and it’s the starting point for all steroid hormones: cortisol, aldosterone, DHEA, testosterone, progesterone, estrogens. In normal times, pregnenolone is distributed fairly between these different synthesis pathways. But in chronic stress situations, the body makes a triage decision. It massively redirects pregnenolone toward cortisol production, at the expense of all other hormones.
It’s a survival choice. Cortisol is the fight-or-flight hormone. For your body, producing cortisol is more urgent than producing progesterone or DHEA. The problem is that when this diversion lasts months or years, the consequences accumulate. Progesterone drops, which creates relative estrogen dominance (even without estrogens increasing). This estrogen dominance increases TBG (thyroid hormone binding protein), which sequesters T3 and T4, making them unavailable for cells. If you’re a woman suffering from painful periods, this mechanism is probably at play. Adrenal fatigue in women is often confused with simple estrogen-progesterone imbalance. DHEA drops, accelerating aging and weakening immunity. Testosterone drops, which worsens fatigue, muscle loss, and decreased libido.
Do you see the picture? Chronic stress doesn’t only block the thyroid directly via cortisol. It also blocks it indirectly by unbalancing the entire hormonal terrain. It’s a domino effect. And the thyroid, situated at the end of the chain, takes a beating without being directly responsible. I’ve seen women in consultation whose thyroid assessment normalized simply by correcting the pregnenolone steal, without touching the thyroid itself. Claire is one of them.
The energy dispatch according to Marchesseau
To go even further in understanding this mechanism, we need to discuss a concept I often use in consultation that comes from Pierre-Valentin Marchesseau, the father of French naturopathy. Marchesseau describes what he calls energy dispatch. The idea is simple but powerful: your body has a finite amount of energy each day, and it distributes it according to an immutable order of priority.
At the top of the list is the mental and nervous sphere. Your brain is constantly consuming, whether it’s working or ruminating. Next comes the digestive sphere, which gobbles up a considerable part of your energy (digesting a heavy meal can monopolize up to forty percent of your available energy). Then locomotion, physical activity. And at the very bottom of the list, relegated to the last rank, elimination and regeneration. Your body only eliminates, repairs, and regenerates when there’s energy left after feeding everything else.
This concept illuminates the stress-adrenals-thyroid link in a way that biochemistry alone cannot. A chronically stressed patient monopolizes the bulk of his energy in the mental sphere. His brain runs in loops, consuming glucose, magnesium, B vitamins, serotonin. To make this nervous energy, the adrenals are constantly solicited: cortisol in the morning to start, adrenaline during the day to keep going, cortisol again in the evening when it should be dropping. There’s nothing left for regeneration, for liver detoxification, for thyroid hormone synthesis. The thyroid slows down not because it’s sick, but because the body has decided it’s not a priority.
This is exactly what Marchesseau described when he talked about the “vacation cold.” You know, that flu that hits you on the first day of vacation? It’s not a coincidence. Your cortical mind finally disconnects, energy gets redistributed, and your body takes the opportunity to do a major cleanup (fever, mucus, fatigue). Your adrenals finally release the pressure, and all the toxemia accumulated over months of stress comes to the surface.
Adrenal fatigue: the diagnosis your doctor refuses
Adrenal fatigue, or partial adrenal insufficiency, is a concept that divides medicine. Conventional endocrinologists only recognize two adrenal states: Addison’s disease (total adrenal insufficiency, a rare and serious illness) and Cushing’s syndrome (excess cortisol). Between the two? Nothing. A diagnostic desert. And yet, it’s precisely in this in-between that millions of exhausted patients whose tests “show nothing” are found.
Dr Lam describes adrenal fatigue in several progressive stages. The first stage is alarm: cortisol rises in response to stress. You feel over-solicited but you manage thanks to adrenaline and coffee. The second stage is resistance: cortisol stays elevated permanently, DHEA starts to drop, the first symptoms appear (disturbed sleep, abdominal weight gain, irritability, sugar cravings). The third stage is exhaustion: cortisol collapses, the adrenals can’t keep up with demand, you’re tired from wake-up, sensitive to everything, unable to handle any additional stress. The fourth stage is failure, close to Addison’s.
Most patients I see in the office are between stages two and three. Their morning blood cortisol, the only one conventional medicine measures, is often “within normal range.” But salivary cortisol at four points during the day (wake, noon, four o’clock, bedtime) tells a completely different story. A study published in Integrative Medicine describes the case of a 49-year-old patient, confirmed Hashimoto, anti-TPO above one thousand units per milliliter (normal is below thirty-five). Her morning salivary cortisol was 49 nanomoles per liter. After a year of adrenal protocol (without touching the thyroid), her cortisol dropped to 18.3 nanomoles per liter, her TSH normalized to 0.48, and her goiter regressed in four weeks. Four weeks. Without any modification to her thyroid treatment. By treating only the adrenals.
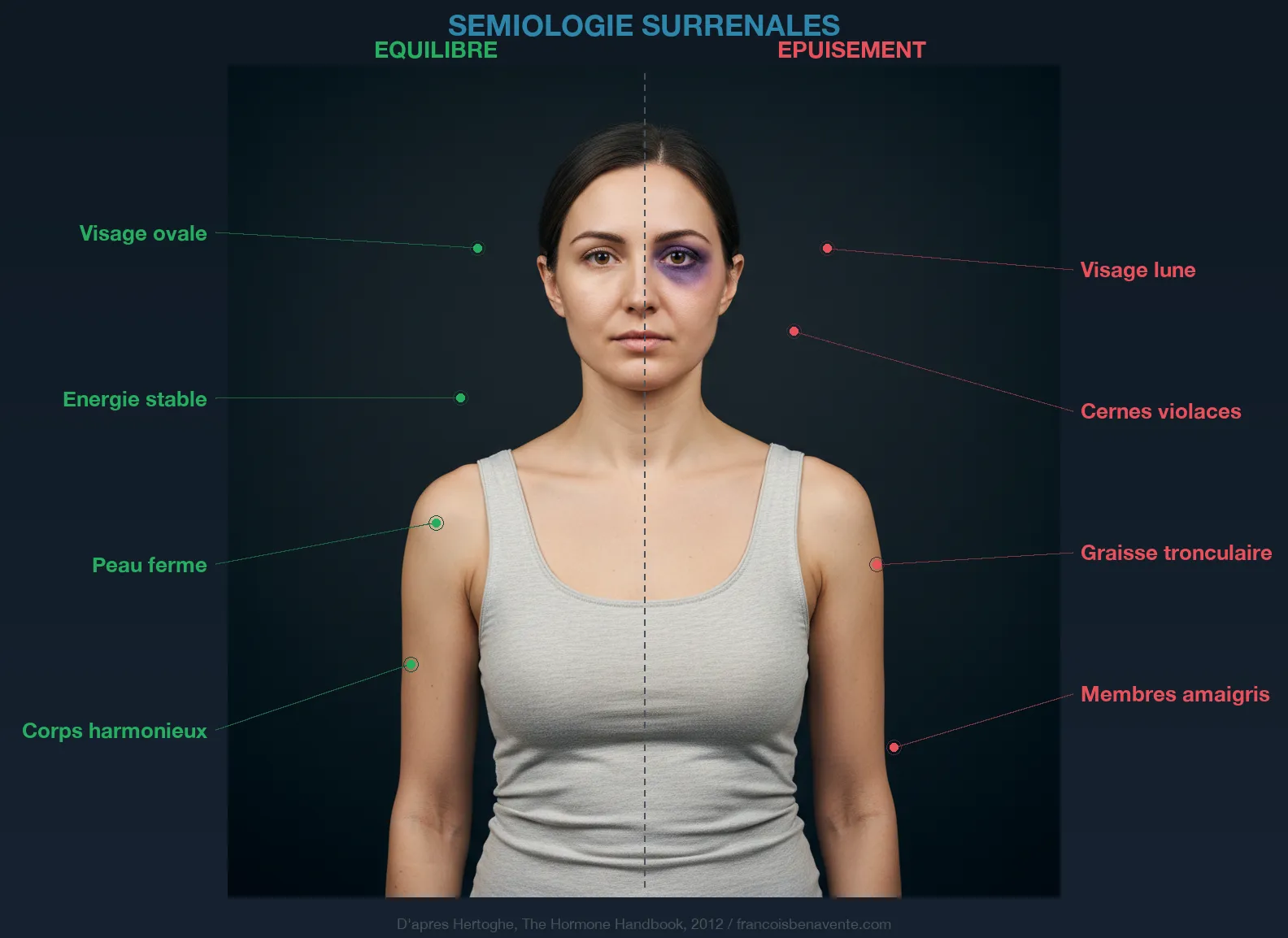
The signs that should alert you are characteristic. A fatigue that doesn’t go away despite rest. A systematic slump between three and five o’clock in the afternoon. An urgent need for coffee in the morning to function, for salt in food. Dizziness when standing up too quickly (orthostatic hypotension). Dark circles even when you sleep enough. Increased sensitivity to cold, noise, light. Recurrent infections (colds that drag on, recurring fungal infections). Non-restorative sleep. And this diffuse sensation that you’re not yourself anymore, that your resilience capacity has evaporated. You can assess your level of adrenal fatigue with the Hertoghe cortisol questionnaire.
Why order is non-negotiable
This is where we arrive at the heart of this article. The question is not only whether your adrenals are tired. The question is: in what order should things be corrected? And the answer is categorical: adrenals first. Thyroid second. Always.
Dr Hertoghe teaches this in his hormone medicine training. Dr Cosserat pounds it in his writings. Dr Lam has made it the pillar of his practice. And I see it every week in the office: giving thyroid hormones to a patient whose adrenals are exhausted makes the situation worse instead of better. Why? Because thyroid hormones accelerate metabolism. That’s their role. They increase oxygen consumption, energy production, cellular demand. But if the adrenals can’t keep up with this acceleration, if they can’t produce enough cortisol to support this metabolic increase, the body panics. The heart races. Anxiety explodes. Insomnia worsens. Fatigue paradoxically gets worse. Some patients describe the sensation of an engine running too fast without oil.
This is why some patients on Levothyrox feel worse after a dose increase. Their doctor, not seeing TSH drop enough, increases the dosage. The patient complains of palpitations, anxiety, tremors, insomnia. The doctor interprets these symptoms as excess T4 and lowers the dosage. The patient falls back into fatigue. The hormonal yo-yo can last years without anyone thinking to look at the adrenals.

The rule is simple: as long as the adrenals aren’t stabilized, any thyroid intervention is at best ineffective, at worst harmful. It’s like trying to repair a car’s engine whose cooling system is broken. You can change the spark plugs, adjust the injection, optimize the fuel, but if the engine overheats, none of that will help.
The three-step protocol
How do you break out of this vicious cycle? My adrenal reconstruction protocol is organized in three stages, and the order is sacred.
The first stage is adrenal restoration. It generally lasts eight to twelve weeks, sometimes longer in severe cases. Magnesium is the first brick: three hundred to four hundred milligrams per day in bisglycinate form, in the evening at bedtime. Magnesium is the number one cofactor for cortisol management. Every cortisol molecule produced consumes magnesium. In chronic stress, reserves collapse. You can assess your deficiency with the magnesium questionnaire. Vitamin C comes next: the adrenals are the organs richest in vitamin C in the human body, and stress is its main consumer. One gram morning and evening in Ester-C or acerola. B vitamins (especially B5, B6, and B12) support cortisol synthesis and neurotransmitters. Rhodiola (two hundred milligrams of standardized extract in the morning) is the adaptogen I prefer in first intention: it normalizes cortisol by raising it when it’s too low and lowering it when it’s too high. Ashwagandha (three hundred milligrams twice daily) completes the picture, particularly effective for the anxiety component and sleep. Licorice, in small doses (two hundred milligrams of extract in the morning, never in the evening, contraindicated in hypertension), slows cortisol degradation and prolongs its effect. For quality supplementation in magnesium, B vitamins, and adaptogens, I recommend Sunday Natural (minus ten percent with code FRANCOIS10).
But supplementation alone isn’t enough if lifestyle continues to drain the adrenals. Sleep is non-negotiable: in bed before eleven o’clock, awake at set time, zero screens an hour before bedtime. Physical activity must be adapted: walking, yoga, swimming, never intense cardio that further exhausts the adrenals (HIIT, CrossFit, long running sessions are prohibited during restoration phase). Diet should be rich in proteins at breakfast (eggs, almonds, avocado) to stabilize blood sugar, which is intimately linked to cortisol. Intermittent fasting, popular as it may be, is often counterproductive in adrenal fatigue because it causes hypoglycemia that forces the adrenals to produce even more cortisol.
The second stage is thyroid evaluation, once the adrenals are stabilized. It’s at this moment, and not before, that I prescribe a complete thyroid assessment: TSH, free T3, free T4, reverse T3, T3L/rT3 ratio, anti-TPO and anti-thyroglobulin antibodies. Why wait? Because the thyroid assessment of a patient in adrenal fatigue is skewed. TSH is artificially low (inhibited by cortisol), reverse T3 is elevated, the T3L/rT3 ratio is collapsed. If you do the test during the adrenal phase, you risk prescribing Levothyrox to a patient who doesn’t need it, or underdosing a patient who does. In a surprisingly high number of cases, the thyroid assessment normalizes spontaneously after adrenal restoration. The patient from the Integrative Medicine study is proof: TSH normalized to 0.48 without modification to thyroid treatment. I observe this phenomenon regularly. Not in every case, but often enough to justify the patience.
The third stage is targeted thyroid optimization. If the post-adrenal assessment reveals persistent hypothyroidism, then we intervene. Correction of cofactors (selenium two hundred micrograms, zinc thirty milligrams, iron if ferritin is low, iodine with caution). Liver support for T4 to T3 conversion (milk thistle, artichoke, rosemary, cellulose-based dinners). Management of endocrine disruptors that block thyroid receptors. I detailed the seven essential cofactors in my dedicated article, and the role of the liver in the article on the liver-thyroid connection.
The most common error I see
The most frequent error, the one I encounter almost every week, is the patient who comes in with Levothyrox prescribed months ago, a “controlled” TSH, and a condition that isn’t improving. When I ask if their adrenals were evaluated, the answer is invariably no. When I prescribe salivary cortisol at four points, results are almost always abnormal. And when we start the adrenal protocol, sometimes without even modifying thyroid treatment, the improvement is spectacular.
Claire, my patient from the beginning of this article, perfectly illustrates this pattern. Her 8 o’clock salivary cortisol was collapsed. Her 4 o’clock cortisol was paradoxically elevated, a sign that the HPA axis had lost its circadian rhythm. After ten weeks of adrenal protocol (magnesium bisglycinate, vitamin C, B complex, rhodiola in the morning, ashwagandha in the evening, bedtime at 10:30 PM, cutting coffee after noon, daily thirty-minute walks), her morning energy returned. The 3 o’clock slump disappeared. Her sleep was restored. And when I checked her thyroid assessment at week twelve, her free T3 had increased by twenty-five percent and her reverse T3 had dropped by half, without any change to her Levothyrox dosage.
The thyroid hadn’t changed. It was the adrenals that had stopped sabotaging it.
I also observe the opposite error, rarer but just as instructive: the patient taking adaptogens and vitamins for their adrenals but refusing to get their thyroid tested. The adrenals and thyroid work in tandem. If the thyroid is truly broken (advanced Hashimoto, thyroidectomy, severe iodine deficiency), the adrenals compensate permanently, and no adaptogen protocol will be able to restore them durably as long as the thyroid isn’t addressed. Dr Claeys writes in End Hypothyroidism that the adrenals are the “firefighters of the thyroid”: they put out fires when the thyroid isn’t warming enough. But even firefighters eventually burn out if the fire never stops.
The digestive clue everyone forgets
There’s one last element I want to address, because it’s systematically absent from articles on stress and the thyroid. Chronically elevated cortisol destroys the digestive lining. It reduces hydrochloric acid production, it slows peristalsis, it weakens the tight junctions of the small intestine. The result? Malabsorption of thyroid cofactors (iron, selenium, zinc, magnesium) and intestinal permeability that opens the door to auto-immunity. I detailed the vicious circle thyroid and digestion in a dedicated article.
In other words, stress doesn’t only block the thyroid through hormonal pathways (cortisol, reverse T3, pregnenolone steal). It also blocks it through the digestive pathway, by preventing the absorption of nutrients it needs to function. This is a third mechanism, less known, but equally devastating. And this is why I always start by assessing digestion in consultation, even when the main concern is the thyroid. How do you expect your supplements to work if your intestines aren’t absorbing anything anymore? That would be like filling a leaky bucket.
The link to weight is obvious. Patients in chronic stress gain weight, especially around the abdomen (cortisol orients storage to the belly via cortisol receptors on visceral adipocytes). This excess weight activates inflammation. Inflammation worsens reverse T3. Reverse T3 slows metabolism. Slowed metabolism promotes storage. Another vicious circle. If you’re in this situation, don’t launch into restrictive dieting. Correct your adrenals first. Weight loss will follow.
What I take away after three hundred consultations
If I had to sum up in one sentence what I’ve learned about the link between stress, adrenals, and thyroid, it would be this: the thyroid is rarely the problem, it’s almost always the victim. Victim of adrenals that slow it down. Victim of the liver that no longer converts. Victim of the intestines that no longer absorb. Victim of stress that diverts the hormonal machinery to its benefit.
The key is order. Adrenals first. Then intestines and liver. Then thyroid. It’s counterintuitive because thyroid symptoms are the most visible (fatigue, weight gain, cold sensitivity, hair loss). It’s tempting to want to correct them first. But if the foundations are cracked, repainting the facade does nothing.
Marchesseau had this formula I like to quote: “The naturopath doesn’t treat disease, he corrects the terrain that allowed the disease to establish itself.” The adrenal terrain is, in my experience, the first terrain to correct in a thyroid patient who isn’t improving despite treatment. If you understand why your doctor refuses to recognize adrenal fatigue, it’s because conventional medicine only knows extremes: Addison or Cushing. But between the two, there’s an entire continent of exhausted patients, underdiagnosed, undertreated, wandering from consultation to consultation searching for an answer nobody gives them.
To understand why Hashimoto complicates this equation even further (the autoimmune component adds a layer of inflammation that worsens reverse T3), read my article on forgotten causes of Hashimoto.
If you recognize yourself in what you just read, if you’re taking Levothyrox without improvement, if your fatigue doesn’t go away despite rest, if you’ve felt “shut down” for months, ask for salivary cortisol at four points. Not morning blood cortisol, which shows nothing. Salivary cortisol at 8 AM, noon, 4 PM, and 10 PM. This simple test can change your understanding of your situation and direct your care in the right direction.
If you want personalized support, you can book a consultation.
To go further
- Magnesium: why your thyroid, your sleep, and your stress depend on it
- Vitamin B5 (pantothenic acid): the vitamin of your adrenals and coenzyme A
- Basedow and stress: the thyroid of emotion
- Burn-out: when your reptilian brain takes control
Want to evaluate your status? Take the Claeys thyroid questionnaire free in 2 minutes.
Want to evaluate your status? Take the Holmes Rahe stress questionnaire free in 2 minutes.
Sources
- Hertoghe, Thierry. The Hormone Handbook. 2nd ed. Luxembourg: International Medical Books, 2012.
- Marchesseau, Pierre-Valentin. Founder of French naturopathy, author of numerous pamphlets (1950-1980).
You can book a consultation for a personalized assessment. I receive in Paris and via video throughout France. Quality adrenal and thyroid supplementation is available from Sunday Natural (minus ten percent with code FRANCOIS10).
Healthy recipe: Golden milk with turmeric: Turmeric and ginger support your adrenals.





Laisser un commentaire
Sois le premier à commenter cet article.