What if your thyroid wasn’t lacking medications, but simply nutritional cofactors? After more than 300 thyroid consultations in my practice, I’m sharing what I observe daily, and what conventional medicine systematically misses.
Is your thyroid really okay?
You’re tired. You feel cold easily. You gain weight for no apparent reason. Your doctor checks your TSH, finds it “within normal range,” and concludes everything is fine. Except it’s not. Hypothyroidism is a symptom, not a diagnosis. I see this scenario every week in my practice. The person across from me knows something is wrong, but their blood work says otherwise. And that’s the beginning of a medical odyssey that can last years.
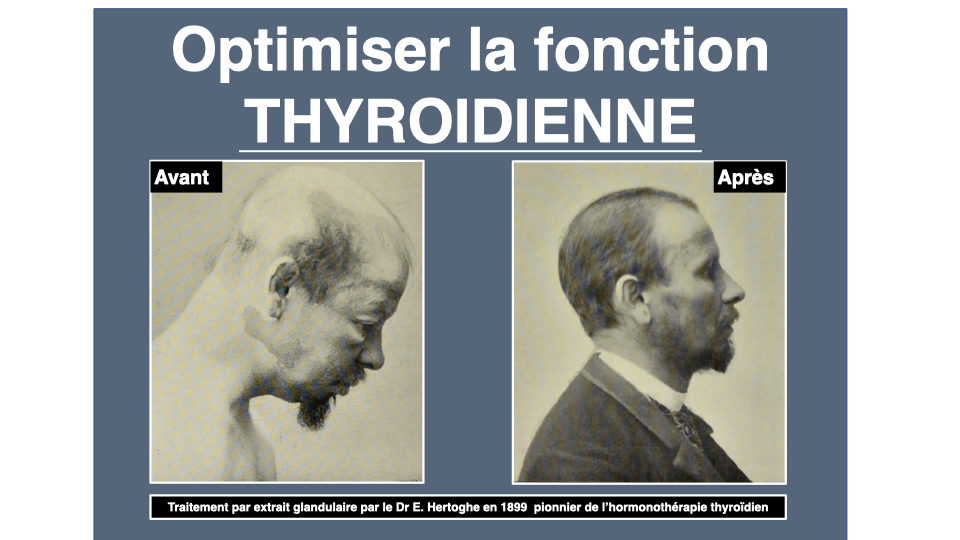
Dr. Eugène Hertoghe described this picture back in 1899. He called it masked myxedema. More than a century later, his great-grandson, Dr. Thierry Hertoghe, keeps hammering the same message in his books and at the Hertoghe clinic in Brussels. As for Dr. Benoît Claeys, he writes in En finir avec l’hypothyroïdie that lab reference ranges only serve to rule out frank pathology, not to define optimal health. The optimal TSH? Below 1.5 mU/L according to biochemist Guénaëlle Abéguilé. Not the 0.4-4.0 that your lab displays as absolute truth.
“Every illness is a reckoning, not an accident; illness is prepared long in advance by errors in hygiene.” Dr V. Pache
The fundamental problem? Medicine too often reduces the thyroid to a single number. TSH + free T4, move along. Yet the production, and especially the conversion of thyroid hormones, depends on specific nutritional cofactors. No cofactors, no conversion. It’s that simple.
What your symptoms are telling you
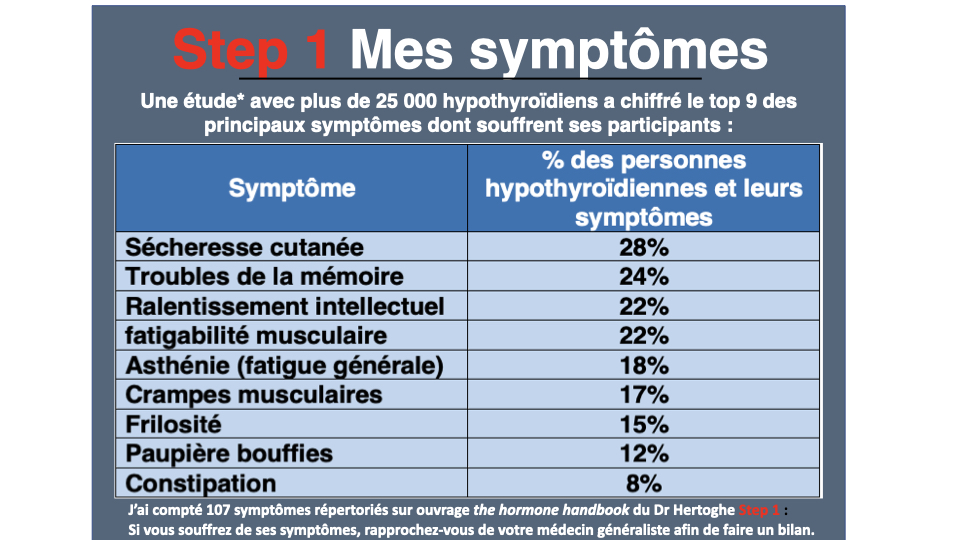
Dr. Hertoghe mapped out hypothyroidism symptomatology in his Textbook with remarkable precision. Chronic fatigue in virtually all cases. Excessive sensitivity to cold in 90% of patients. Bradycardia in 95%. Dry, thickened skin. Loss of the outer third of the eyebrow, that famous Hertoghe sign that I teach in my courses and that too few doctors know about. Constipation. Weight gain despite controlled eating. Depression. Brain fog. Hair loss.
What I observe in my clients? The profile is always the same. People spending most of their days indoors. Lack of sunlight. Lack of fresh air. Chronic stress. Cooked, ultra-processed food, often driven by emotion. Poor sleep quality. In short: an oxidized, deficient, and stressed terrain. The thyroid is just the indicator.
I think of Nathalie (name changed), 45, who came to consult me last year. TSH at 3.2 mU/L, “within normal range” according to her doctor. But her free T3 was low at 2.8 pmol/L (the target is above 5.2 pmol/L according to Cosserat), her ferritin at 22 ng/mL, her plasma selenium at 65 µg/L, her 25-OH-D at 18 ng/mL. Her endocrinologist had told her everything was fine. After four months of targeted nutritional correction, her free T3 rose to 4.1 pmol/L and her symptoms clearly improved. No Levothyroxine. Just the right cofactors, at the right time.
My thyroid strategy in 4 axes
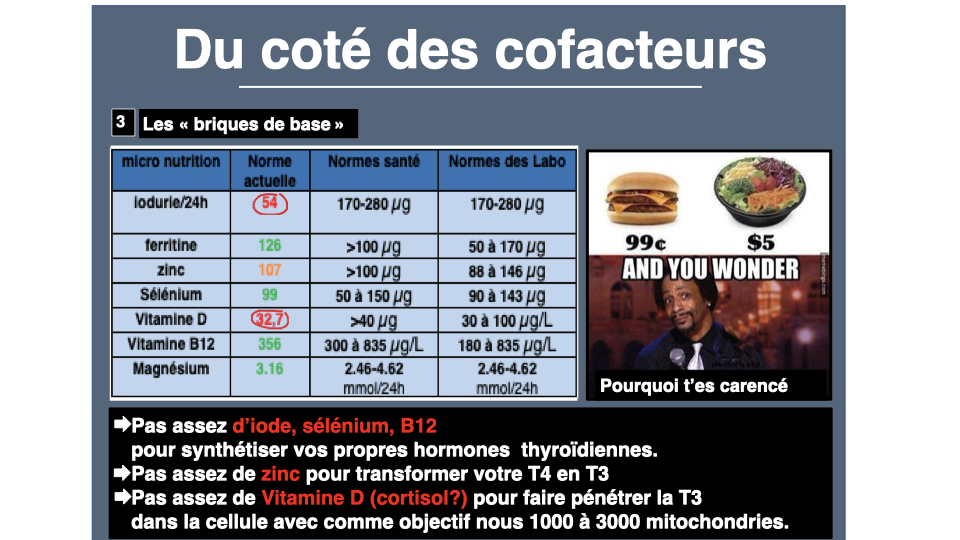
In all my BHV (vital hygiene assessments), I use a four-axis framework. The first is the foundation brick: nutrients essential for thyroid function. Iodine, tyrosine, magnesium, vitamin D, iron, zinc, copper, vitamins A and E. Without these bricks, the thyroid simply cannot synthesize its hormones.
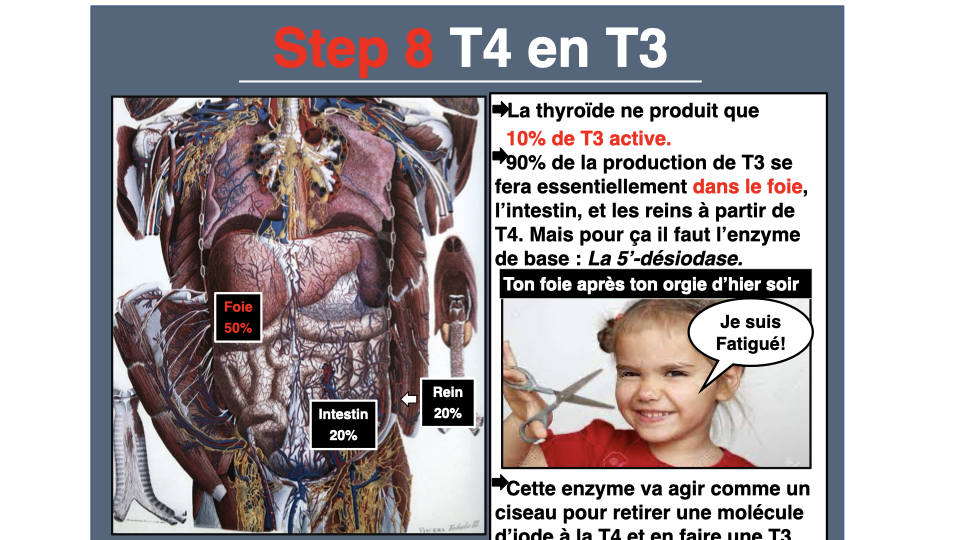
The second axis covers the cofactors for T4 to T3 conversion. The thyroid produces essentially T4 (thyroxine), a relatively inactive pro-hormone. It’s in the liver and kidneys that T4 transforms into T3, the active form, thanks to an enzyme called 5’-deiodinase. And this enzyme needs selenium, iron, molybdenum. It also needs a healthy liver and a functional intestinal ecosystem. Think of it like a car: you have fuel in the tank, but the injector is stuck.
The third axis concerns cellular reception. Even if T3 is present in the blood, it still needs to penetrate the cells. For this, you need to correct deficiencies in vitamin D3, omega-3, eliminate excess colloidal waste (Salmanoff, in his capillary theory, spoke of 5 kg of waste for a 54 kg body), and above all correct the poor estrogen/progesterone balance. Excess estrogens increase TBG, the transport protein, which sequesters thyroid hormones and prevents them from working.
The fourth axis covers the factors that harm the thyroid mechanism: deficiencies of all kinds, metabolic syndrome, tea/coffee/dairy products/cigarettes/gluten (which prevent T4 to T3 conversion), bad DIO2 gene (Dr. Georges Mouton showed on 1,704 patients that 13.4% are homozygous variants), heavy metal or fluoride poisoning.

The 7 nutrients your thyroid depends on
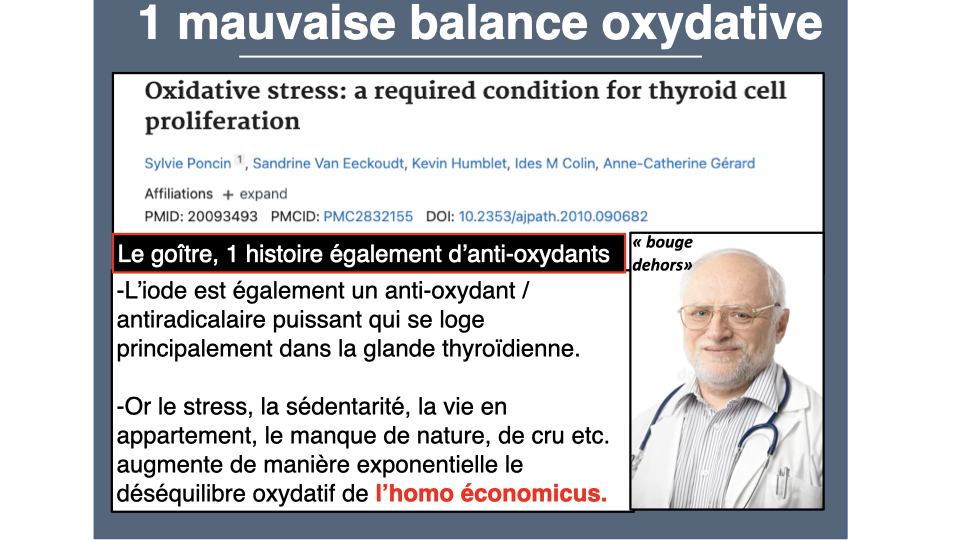
Selenium first. The thyroid is the tissue with the highest selenium content in the entire body, per gram of tissue1. The human selenoprotein genome is encoded by 25 genes2: glutathione peroxidases, superoxide dismutase, thioredoxin reductase. These enzymes protect the thyroid from oxidative stress generated by its own activity (H₂O₂ production is necessary for hormone synthesis). In supplementation, selenomethionine at 100-200 µg per day remains the gold standard, especially in autoimmune thyroiditis3.
Zinc is involved in more than 300 enzymatic reactions. Prof. Jean Lederer from Louvain University and Dr. Benoît Claeys have described in detail the zinc-thyroid link. According to Claeys, more than 90% of patients in consultation have a clear zinc deficiency. Zinc is essential for thyroid hormone synthesis AND for T4 to T3 conversion4. A zinc deficiency means T3 cannot penetrate cells. Worse: supplementing T3 in a zinc-deficient patient can cause heart palpitations, because the heart is more sensitive to T3 than other tissues. Claeys goes so far as to write that the majority of thyroid hormone treatment failures result from zinc deficiency. You can assess your status with the zinc deficiency questionnaire.
Iron, same story. Thyroperoxidase (TPO) is an iron-dependent enzyme5. Without sufficient iron, hormone synthesis stalls6. But free iron is pro-oxidant (Fenton reaction). Never supplement blindly. Always check ferritin first, and aim for between 50 and 80 ng/mL. You can assess your deficiency signs with the iron questionnaire.
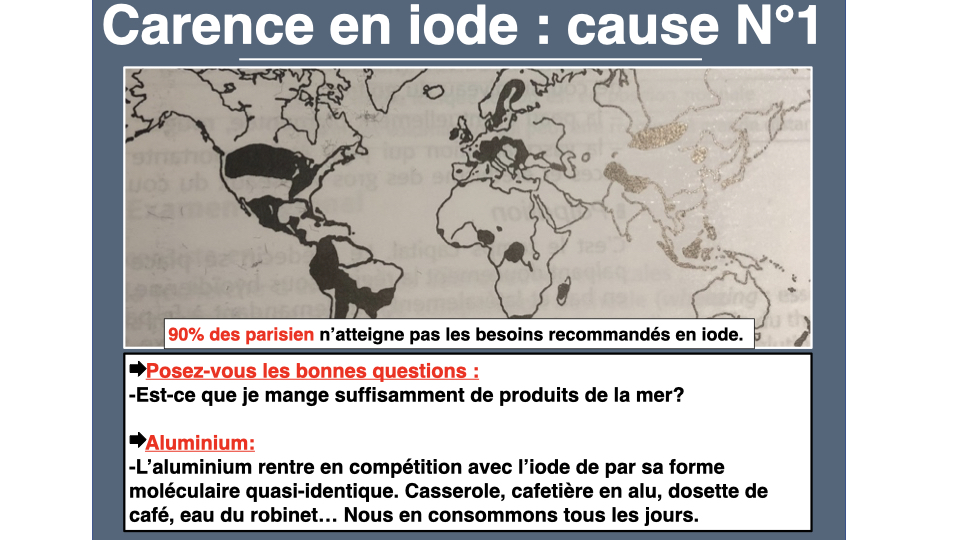
Iodine, the fundamental fuel. T4 contains four iodine atoms, T3 contains three. The human thyroid contains 12 to 16 mg. Dr. Didier Cosserat recommends 150 micrograms per day for adults, 200-250 for pregnant women. A quality iodine supplement or marine algae (wakame, nori, kelp) cover these needs. Sea salt and Himalayan salt contain only traces, contrary to popular belief. But be careful: in autoimmune thyroiditis, excess iodine can worsen the autoimmune mechanism in Hashimoto’s patients. I’ve devoted a complete article to the question of iodine and thyroid autoimmunity. The key is oxidative balance: you must first correct selenium, vitamins A, D, E, and K2 status before supplementing with iodine. Iodine has an inseparable partner: L-tyrosine, an amino acid that is the direct precursor of thyroid hormones and also of dopamine. This explains why so many hypothyroid people also lack motivation and drive.
Vitamin D. About 80% of French adults show insufficiency (ENNS study, Vernay et al., 2012). Yet Hashimoto’s thyroiditis, the leading cause of hypothyroidism in France, is an autoimmune disease. And vitamin D is a precursor to glutathione, our main endogenous antioxidant. Aim for a 25-OH-D level above 60 ng/mL, well above the usual “you’re within normal range.” 2,000 to 4,000 IU per day of vitamin D3. You can assess your deficiency with the vitamin D questionnaire.
And magnesium, universal cofactor, is involved in T4 to T3 conversion, in thyroid receptor sensitivity, and in ATP production. Carnitine, often overlooked, also plays a key role in transporting fatty acids to the mitochondria and in the cellular energy of hypothyroid patients. In other words: in everything that’s lacking in tired, cold-sensitive hypothyroid patients. In magnesium bisglycinate, 300 to 400 mg in the evening. You can assess your deficiency with the magnesium questionnaire.
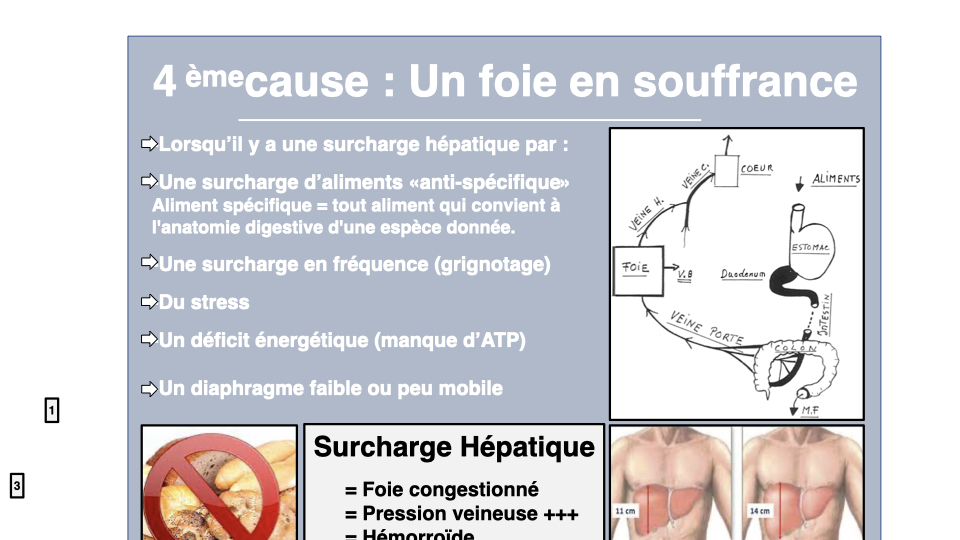
The liver, the thyroid’s forgotten organ
The liver-thyroid relationship is bidirectional. The liver is the primary site for T4 to T3 conversion via deiodinases. It synthesizes TBG, the transport protein. It metabolizes excess estrogens that block the thyroid. And it regulates cholesterol via HMG-CoA reductase, an enzyme directly activated by T3.
In the hypothyroid person, this enzyme runs slowly. Consequence: LDL cholesterol accumulates (reduced clearance), bile acid conversion decreases, bile becomes saturated, and gallstones form. How many of my clients were prescribed statins for cholesterol that was merely the reflection of a struggling thyroid?
Non-alcoholic fatty liver disease (NAFLD) is also common in hypothyroidism. Fatty liver, metabolic syndrome, insulin resistance: it’s a vicious cycle where the thyroid slows the liver and the liver slows the thyroid. Hence the importance of systematically including a liver component: cellulose dinners two evenings per week (carrot, turnip, black radish, artichoke), ginger-rosemary decoction in the morning, support with sulforaphane and indole-3-carbinol from cruciferous vegetables. This is the logic of detoxification applied to thyroid terrain.
What sabotages your thyroid daily
Xenobiotics deserve serious attention. According to EFSA (2013), 101 pesticides out of 287 evaluated affect the thyroid7. Inhibition of synthesis, disruption of metabolism, disruption of transport: xenobiotics attack at every level. PCBs, dioxins, phthalates, bisphenols, perchlorates, and thiocyanates, the list is long. And some of these endocrine disruptors hide directly in your kitchen utensils.
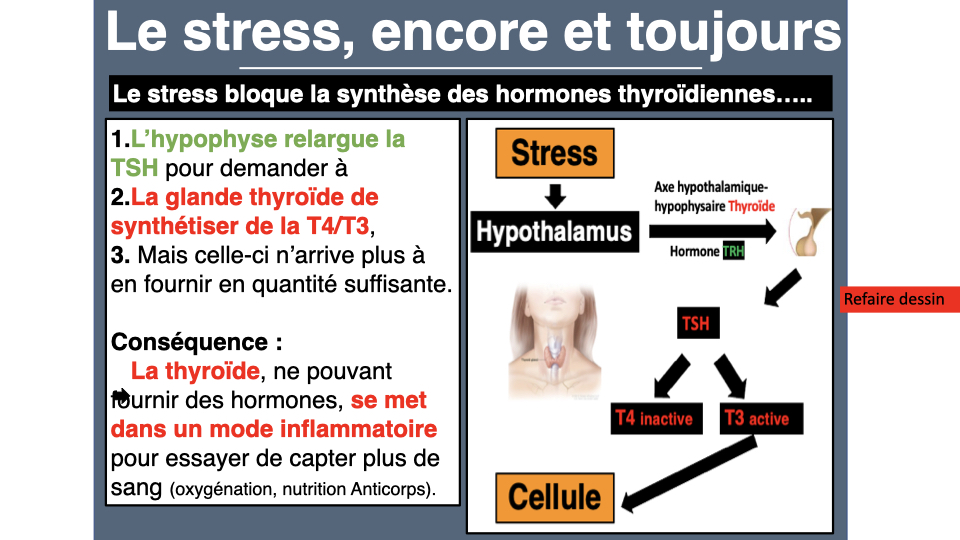
Chronic stress diverts pregnenolone toward cortisol at the expense of progesterone and thyroid hormones. This pregnenolone theft is also one of the major causes of menstrual cycle disorders, where progesterone deficiency fuels relative hyperestrogenism. Masked hypothyroidism also worsens PCOS by slowing ovulation. Adrenal fatigue is perhaps the most frequent cause of thyroid insufficiency, as Dr. Michael Lam explains. If you treat the thyroid BEFORE the adrenals, active T3 converts to reverse T3 (inactive). Always treat the adrenals first; that’s a rule I apply systematically.
Sleep too. After six days of sleeping 4 hours, the TSH curve flattens8. Sleep deprivation literally crushes the thyroid axis. Tryptophan chronobiology, serotonin-melatonin, and morning light therapy play a direct role in T4 to T3 transcription.
The complete tests to demand
Dr. Didier Cosserat recommends a thyroid assessment far beyond simple TSH + free T4. Here’s what I systematically request: free T3, free T4, reverse T3, free T3/reverse T3 ratio (which should be above 0.015), anti-TPO and anti-thyroglobulin antibodies, urinary iodine, TBG, selenium, ferritin, zinc, vitamin D, urinary cortisol, urinary magnesium. And in advanced cases: homocysteine, folates, ultra-sensitive CRP, total glutathione, SOD, GPX for oxidative balance.
Want to assess your thyroid function? The Claeys questionnaire is a good starting point. If you suspect associated adrenal exhaustion, complete it with the Hertoghe cortisol test.
Basal oral temperature upon waking remains a valuable indicator: below 36 degrees, hypothyroidism should be suspected. The objective is 36.6 degrees. In women, measurement is taken at day 2 of the cycle (Wilson test).
What to do practically
“Hippocrates’ theory of contraries is the foundation of all our practice: identify what is lacking and supply it, identify what is in excess and reduce it.” Pierre-Valentin Marchesseau
Before any pill, the plate. Algae (wakame, nori, kombu) for iodine. Brazil nuts for selenium. Oysters for zinc and iron. Fatty fish for vitamin D. Leafy greens for magnesium. Quality animal proteins for tyrosine. This is what Dr. Hertoghe calls the Optimal Hormone Diet. Anti-inflammatory eating takes on full meaning here: cleanse first, nourish second.
If testing confirms deficits, and only then, targeted supplementation. Selenomethionine 100-200 µg/day in case of autoimmune thyroiditis. Zinc bisglycinate 15-30 mg with 2 mg copper. Iron bisglycinate only if ferritin is under 50. Vitamin D3 2,000-4,000 IU/day to reach 40-60 ng/mL. Magnesium bisglycinate 300-400 mg in the evening. L-tyrosine 500-1,000 mg in the morning on an empty stomach. Minimum three to six months before re-evaluation.
And lifestyle always. Micronutrition without lifestyle is like putting premium gas in a clogged engine. Heart coherence for stress. Seven to eight hours of sleep, in bed before 11 p.m. Thirty minutes of natural light each morning. Strength training, which stimulates T4 to T3 conversion in muscle. And above all: never stop Levothyroxine or Cynomel treatment without medical advice. Micronutrition supports the terrain. It doesn’t replace a medical diagnosis.
You all have a plant at home struggling to survive however it can. When it yellows, you don’t treat it. You change its conditions. More light, more water, better soil. Your thyroid is exactly the same thing. Assess, correct, re-evaluate. And above all, never neglect the terrain.
For thyroid micronutrition, Sunday Natural offers selenium, zinc, natural iodine, and quality pharmaceutical B vitamins (-10% with code FRANCOIS10). A Hurom extractor prepares mineral-rich green juices for thyroid health (-20% with code francoisbenavente20). And the Inalterra grounding mat reduces the inflammation that slows T4/T3 conversion (-10% with code FRANCOISB). Find all my partnerships with exclusive promo codes.
Scientific references
If you want personalized support, you can schedule a consultation.
For more information
- Hertoghe Diet: the dietary protocol that optimizes your thyroid
- Hypothyroidism is a symptom, not a diagnosis
- Thyroid and digestion: the vicious cycle no one explains to you
- NAC and glutathione: the shield nobody prescribes
Sources
- Hertoghe, Thierry. The Hormone Handbook. 2nd ed. Luxembourg: International Medical Books, 2012.
- Mouton, Georges. Écologie digestive. Marco Pietteur, 2004.
- Salmanoff, Alexandre. Secrets et sagesse du corps. La Table Ronde, 1958.
- Vernay, M. et al. “Vitamin D Status (ENNS).” Urology Annals 4, no. 3 (2012): 163-172.
“We rebuild every human being with food, baths, and exercise. The rest is utopia.” Pierre-Valentin Marchesseau
Footnotes
-
Ventura M, Melo M, Carrilho F, “Selenium and Thyroid Disease: From Pathophysiology to Treatment,” International Journal of Endocrinology 2017 (2017): 1297658. PMID: 28255299. ↩
-
Kryukov GV, Castellano S, Novoselov SV et al., “Characterization of Mammalian Selenoproteomes,” Science 300, no. 5624 (2003): 1439-1443. PMID: 12775843. ↩
-
Drutel A, Archambeaud F, Caron P, “Selenium and the Thyroid Gland: More Good News for Clinicians,” Clinical Endocrinology 78, no. 2 (2013): 155-164. PMID: 23046013. ↩
-
Nishiyama S, Futagoishi-Suginohara Y, Matsukura M et al., “Zinc Supplementation Alters Thyroid Hormone Metabolism in Disabled Patients with Zinc Deficiency,” Journal of the American College of Nutrition 13, no. 1 (1994): 62-67. PMID: 8157857. ↩
-
Hess SY, Zimmermann MB, Arnold M et al., “Iron Deficiency Anemia Reduces Thyroid Peroxidase Activity in Rats,” Journal of Nutrition 132, no. 7 (2002): 1951-1955. PMID: 12097675. ↩
-
Zimmermann MB, Kohrle J, “The Impact of Iron and Selenium Deficiencies on Iodine and Thyroid Metabolism,” Thyroid 12, no. 10 (2002): 867-878. PMID: 12487769. ↩
-
Leemans M, Couderq S, Demeneix B, Fini JB, “Pesticides With Potential Thyroid Hormone-Disrupting Effects: A Review of Recent Data,” Frontiers in Endocrinology 10 (2019): 743. PMID: 31920955. ↩
-
Spiegel K, Leproult R, Van Cauter E, “Impact of Sleep Debt on Metabolic and Endocrine Function,” Lancet 354, no. 9188 (1999): 1435-1439. PMID: 10543671. ↩



Laisser un commentaire
Sois le premier à commenter cet article.